

Authors
|
|||||||||
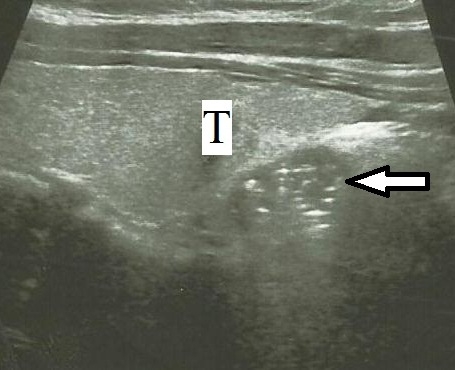
AbstractBronchogenic cysts are originated from the abnormal budding of the tracheobronchial tree during embryogenesis. These are cysts that seen in mediastinum mostly and appear in cervical region rarely. Patients are usually asymptomatic but when the cyst compresses adjacent structures or is infected, they may present with stridor, pain, cough, or dyspnea. Herein, a 47 year-old woman with sore throat and pain at thyroidal region who was referred by the endocrinologist to our clinic is presented.IntroductionIt is believed that bronchogenic cyst (BC), a rare congenital anomaly, results from abnormal budding of the ventral foregut which constitutes tracheobronchial tree later on [1-5]. It’s commonly seen in mediastinum and pulmonary parenchyma, but neck is a relatively unusual site for BCs [1,6,7]. Majority of BCs are diagnosed in pediatric age group [2,4]. Patients are usually asymptomatic. However, as the cyst compresses adjacent structures or is infected, they may present with stridor, pain, cough, or dyspnea [6]. Most of BCs are incidentally detected on radyograms [1,7]. Uniloculation and liquid fluid are frequently-encountered features of these cysts but hemorragic liquid or air may also be seen [4]. Herein we present a bronchogenic cyst that appears as perithyroidal cyst. Case ReportA 47 year-old woman with sore throat and pain at thyroidal region was referred by the endocrinologist to our clinic. Physical exam showed no any palpable neck mass. Ultrasonography revealed a 17x11 mm, heterogen cystic mass with multipl calcification in right infrahyoideal area (Figure 1).
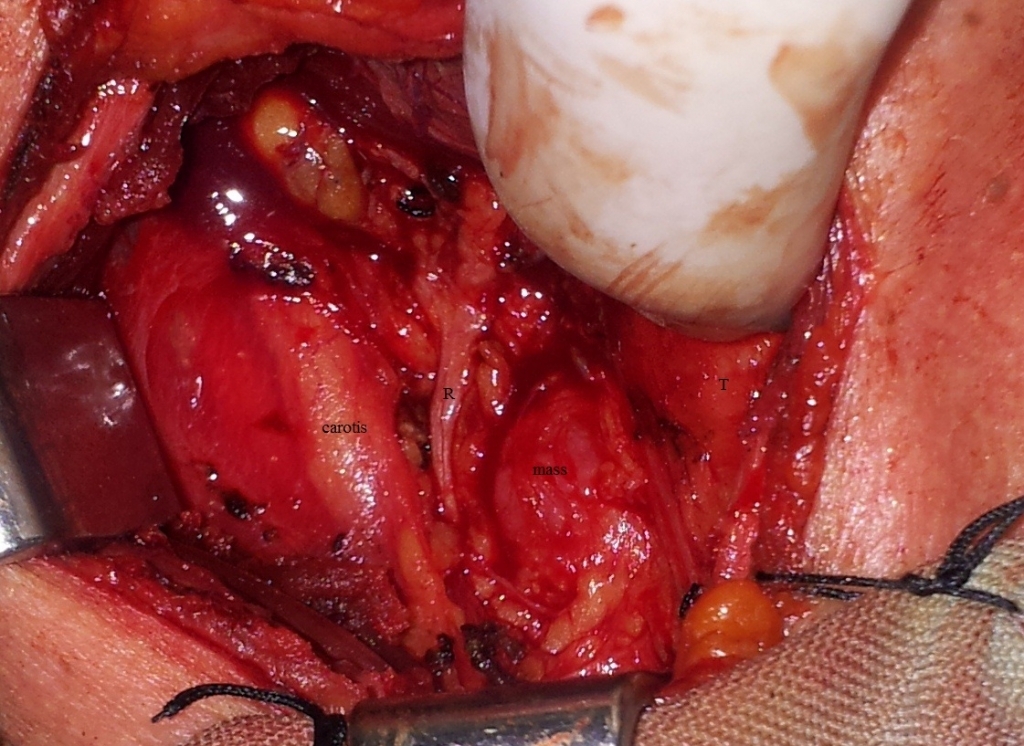
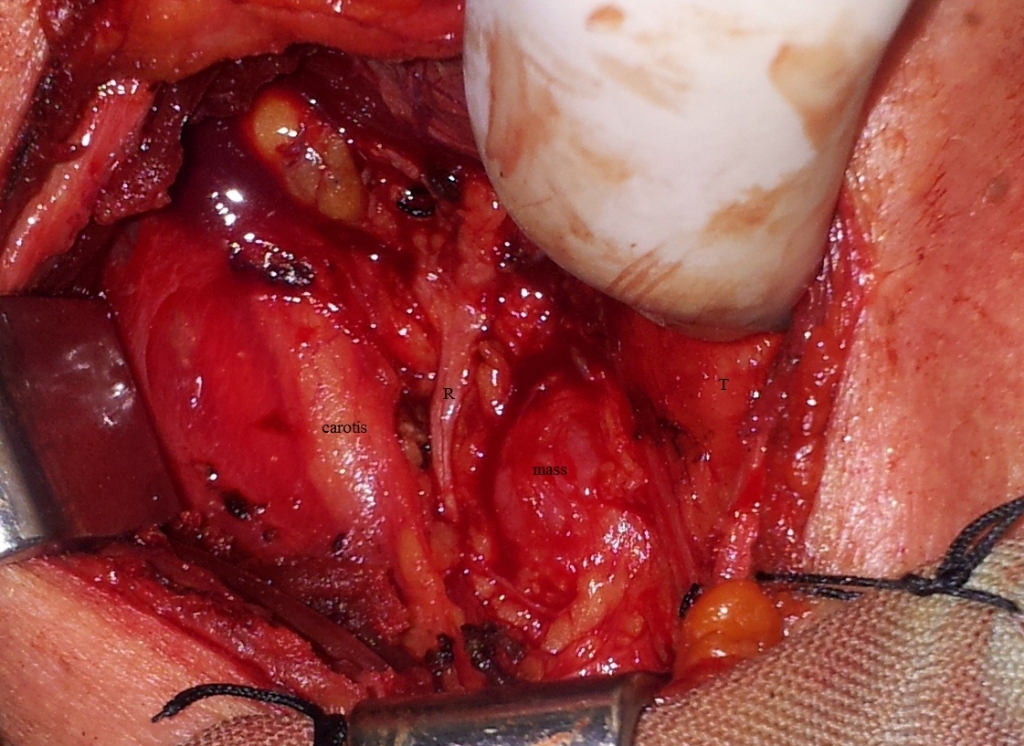
Her thyroid function tests (Thyroid-Stimulating Hormone, free T3 and free T4), calcium and parathormone levels were in normal range. Fine needle aspiration didnot give a definite diagnosis. Neck exploration was planned. First of all, right hemithroidectomy was performed, then recurrent nerve and parathyroid glands were identified. A 2 cm-cystic mass tightly adherent to trachea and esophagus was inbetween right recurrent nerve and trachea, excised with meticulous dissection and the site of origin was sutured (Figure 2-3).
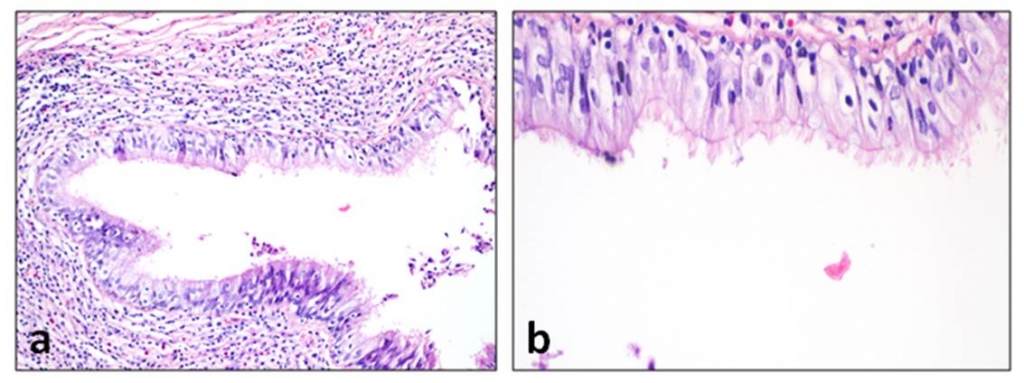
Pseudostratified ciliated columnar epithelium fitted multipl cystic spaces on histopathologic examination, pointed as bronchogenic cyst (Figure 4). Postoperative recovery was uneventful and no recurrence was observed at sixth month.
DiscussionBCs are rare, benign, congenital lesions and although its more common in children, they can be seen in adult age [4]. Primitive foregut divides to form the ventral trachea and dorsal esophagus during fourth-fifth week of embryologic development. As a result of abnormal budding of the ventral foregut, BC occurs (8). Buds can migrate abnormally during development and appear intrathoracic or extrathoracic regions such as abdomen, retroperitoneal, subcutis or neck [4,8]. Maier (9) classified BCs into five groups according to their site of origin; paratracheal, carinal, hilar, paraesophageal and atypic. We met only three cases which limited to the tracheo-esophageal groove in the literature; Bocciolini et al. [4], Sanli et al. (10) and Al-kasspooles et al. [11] presented 57 year-old man with right sided 5x4 cm, 48 year-old woman with right sided 3x2 cm and 62 year-old man with 7x4 cm bronchogenic cysts respectively. Definitive diagnosis can only be made with histopathologic evaluation [1,7]. Cyst epithelium is pseudostratified ciliated columnar epithelium and may contain goblet cells. Sometimes squamous epithelium can be seen secondary to infections [4]. Histologically cyst wall may include smooth muscles, mucous glands and cartilage like in bronchus [1]. In the differential diagnosis of the cystic neck masses, branchial cleft cysts, thyroglossal duct cysts, parathyroid cysts, cervical tymic cysts, cystic hygromas, and cystic neuromas should be kept in mind [1,5,6]. Localization and histology are very important for determining these lesions [2,4]. The patient was consulted to our clinic with suspicion of carcinoma at paratyhroid area because of multiple calcifications in the mass. Majority of the parathyroid carcinomas are functional and high levels of both parathormone and calcium are encountered at laboratory tests [12]. On the other hand, another type of those tumors is non-functional type and together with normal laboratory findings. Usually parathyroid carcinomas are solid lesions and seem as adenomas [13]. A parathyroid carcinoma emerged as a cystic neck mass was reported by Pirundini et al [14]. In our case, there was a cystic mass at parathyroid region with normal calcium and parathormone levels, so we think that carcinoma is a conceivable prediagnosis. Another misdiagnostic factor was sonographic multiple calcified content of the mass which led us to suspect malignancy. But BC's calcific densities are known and it’s thought that high calcium content cause these lesions [15]. Definitive treatment for BCs is complete surgical removal [1,3,5] but there is no need for wide resection [7]. In some cases, carcinoma were reported on the ground of these cysts in the literature. Tanaka et al. (16) reported mucoepidermoid carcinoma which originated from thymic bronchogenic cyst in a 59 year-old woman and Tanita et al. [17] informed malign melanoma case arising from a scapular cutaneous BC in a 46 year-old man. We believe that these congenital cysts have to be excised when they are encountered because of their malign potential. In conclusion, in the differential diagnosis of cystic neck masses, BCs must be kept in mind and complete resection of these lesions should be performed because of their malign potential. References
Presented atThis case report was presented as poster presentation at 36. Turkish National Congress of ENT and Head-Neck Surgery in Antalya/Turkey, in 2014. |
|||||||||
| Keywords : Bronkojenik kist , Kistik kitle , Boyun , Peritiroidal kitle | |||||||||

|