

Authors
|
|||||||||||
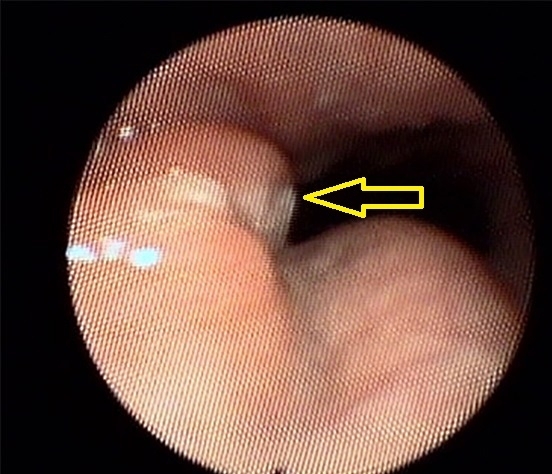
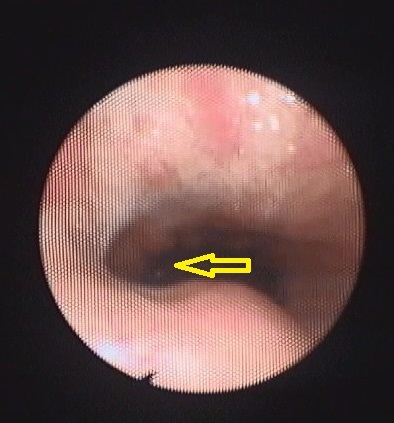
AbstractEpidermoid cysts are benign, slow growing masses that derived from abnormal development of ectodermal tissue. Dermoid and epidermoid cysts are rarely seen in oral cavity and mostly presented in the 1st year of life. In this case we presented an adult patient who had an unusual mass in soft palate which was diagnosed as epidermoid cyst.IntroductionEpidermoid cysts are cutaneous cysts which is surrounded by squamous epithelium without any adnexial structures [1]. Almost 7 % of them present in head and neck region and only 1.6 % of them appear in oral cavity [2]. Epidermoid cysts represent less than 0.01 % of oral cavity cysts and mostly seen in young to middle aged adults [3]. These cysts generally occur in the floor of the mouth but rarely presented in soft and hard palate [2]. The soft and hard palate epidermoid cysts are mostly seen in infants or newborns and generally diagnosed by inspection [4-8]. In this paper we presented a case with an epidermoid cyst of soft palate that causes nasopharyngeal obstruction. Case ReportA 49 year-old women admitted the otolaryngology clinic of our tertiary academic center with the complaint of snoring. Her BMI was 22.1. She had nasal septal surgery 3 months ago but snoring was present. In direct oropharyngeal examination there was no tonsillar hypertrophy or asymmetry of soft palate. Flexible fiberoptic nasopharyngoscopy revealed a right sided lateral bulging causing asymmetric nasopharyngeal obstruction (Figure 1).
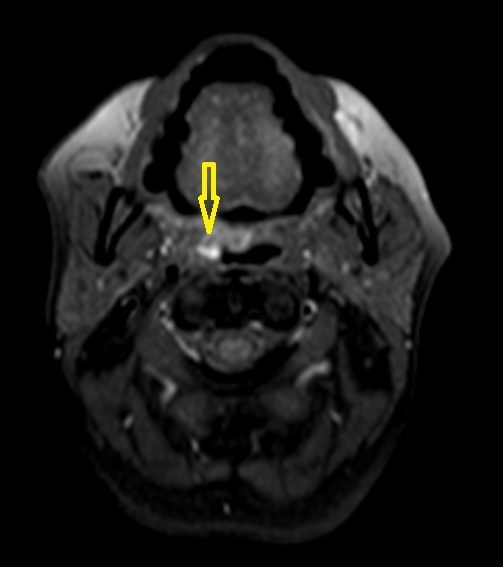
Then we performed magnetic resonance imaging (MRI) which showed a 6 mm in size, ovoid shaped mass located right side of the uvula in soft palate. In T1A and T2A sections it was hyperintense and it was not contrast enhancing (Figure 2).
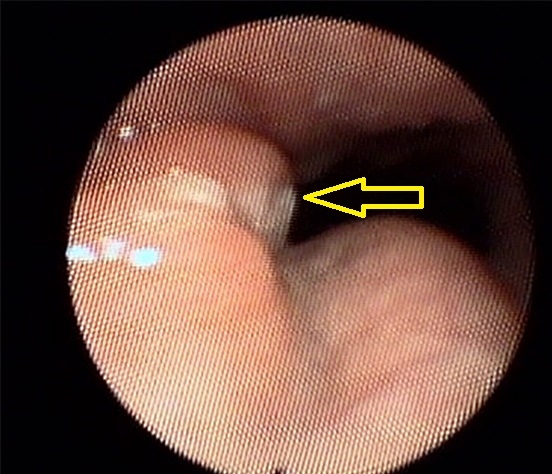
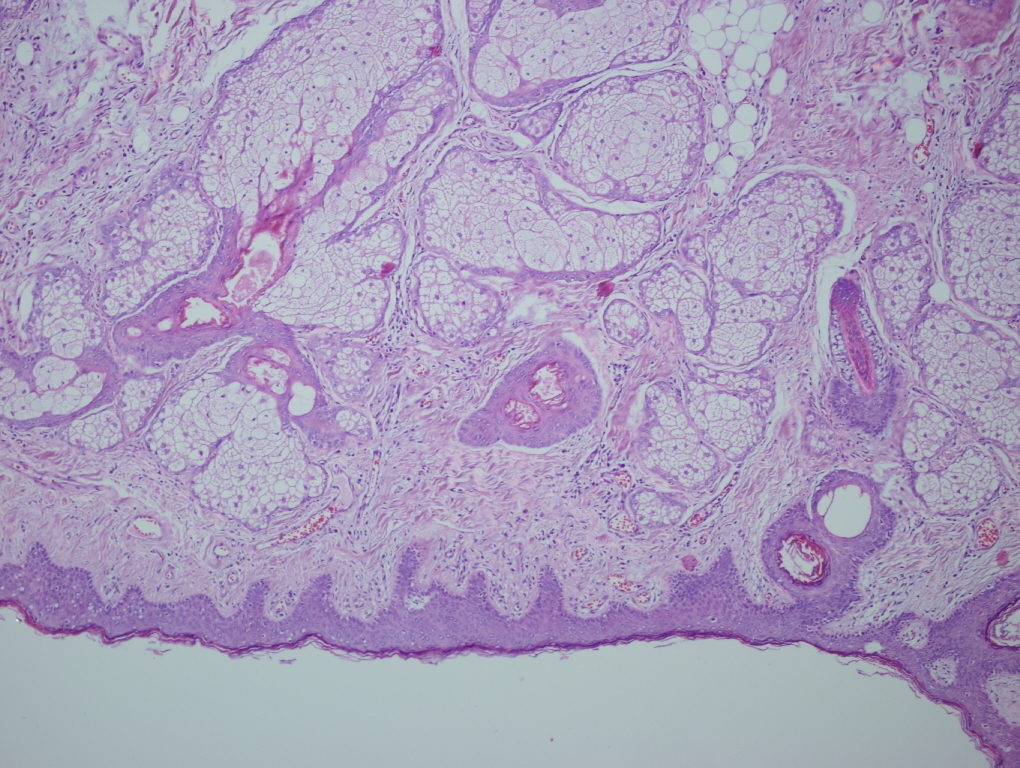
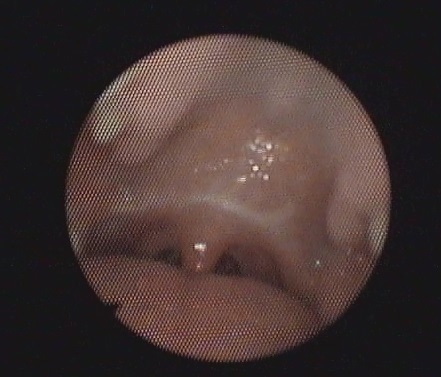
Surgical removal in general anesthesia was planned and an informed consent was obtained. A transpalatal approach was performed and we reached the solid mass through a 2 cm incision. The mass was dissected from the surrounding palatal muscles and en-bloc removed. Palatal muscles and the mucosa were sutured by 4/0 vicryl to close the space. Macroscopically it was 2 cm long, whitish colored semisolid mass. Histologically the mass was consisted of cyst, lined with keratinized squamous epithelium surrounded by fibrous connective tissue and filled with keratin debris (Figure 3). The patient’s complaint of snoring was ended and nasopharyngeal obstruction was disappeared in postoperative nasopharyngoscopy 3 months after surgery (Figure 4,5).
DiscussionAlthough a few cases of malignant transformation of epidermoid cysts have been reported, they are benign, slow growing masses [9,10]. Seven percent of epithelial cysts presented in head and neck region and only 1.6 % of them are located in the oral cavity [2]. Epidermoid cysts can be classified as congenital or acquired regarding to its generation [11]. During embryological development congenital inclusion of ectodermal tissue may result a cyst formation. Other theory suggests the implantation of epithelial tissue into deep mesenchymal tissue by surgical or accidental trauma [12]. It is presumed that ectodermal sequestration during first and second branchial arches' development results with midline cysts and fusion of the lateral processes of the branchial arches may induce the formation of cysts in the oral cavity [13,14]. Epidermoid cysts generally diagnosed incidentaly and remain asymptomatic [5]. The clinical presentation of an intraoral epidermoid cyst is related to its size and site of origin. The epidermoid cyst of oral cavity may cause obstructive sialodenitis [15] or the epidermoid cyst in the floor of the mouth may cause a life-threatening airway obstruction [16]. Published cases of dermoid and epidermoid cysts of the palatal region were presented generally in the first year of life [7]. Zappia et al. presented an epithelial inclusion cyst of a 62 year-old patient located at the soft palate who underwent a prior uvulopalatopharyngoplasty [17]. In this case of Zappia et al. the patient had a previous trauma to palatal region and here the theory of implantation of epithelial tissue is valid. But in the case that we presented here, the patient did not have any previous surgical procedure to the palatal site. The depth of the mass and no histologic finding of a foreign body supports the congenital theory. This case report emphasizes the importance of nasopharyngeal endoscopy in differential diagnosis of other obstructive upper airway pathologies that causes snoring. Surgical removal of the cystic mass is the preferred choice of treatment. The differential diagnose of the cysts of the uvulopalatal region include dermoid cysts, teratomas, mucoceles, branchial cleft cysts [2]. In conclusion, when examining a snoring patient, flexible fiberoptic nasopharyngoscopy should be performed especially for the individuals with a normal looking palate in case of an epidermoid cyst of soft palate. References
Presented at12th Turkish Rhinology Congress |
|||||||||||
| Keywords : Epidermoid kist , Yumuşak damak , Horlama | |||||||||||
|