

Authors
|
|||||||||
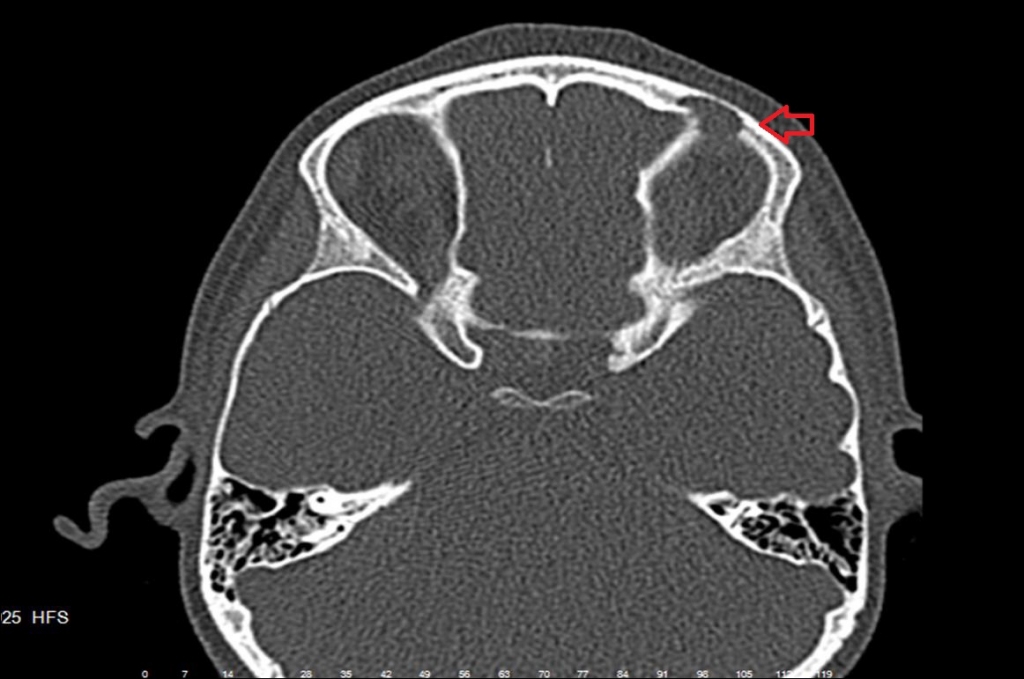
AbstractLangerhans cell Histiocytosis (LCH), is a disease characterized byabnormal proliferation of langerhans cells in various tissues and organs. The primary lesion is consistent with various number of macrophages, lymphocytes and pathological langerhans cells which is characterized by a clonal poliferation of Langerhans cells. LCH can be seen at any age but it makes peak in 1-3 years of age and especially in men twice more often than women. The etiology is unknown, although many factors (infection, heredity, trauma, etc.) are thought to play a role in the etiology. Aproximately 60% of patients are presented with head and neck involvement and often with skull base involvement. Here, we want to present a case of LCH mimicking preseptal cellulitis as a sinusitis complication. IntroductionLangerhans cell histiocytosis (LCH) is a clonal proliferative disease of Langerhans cells that express an immunophenotype positive for S100 CD1a and Langerin (CD207), and which contain cytoplasmic Birbeck granules. Disease expression ranges from mild to severe disease [1]. The cause of this disease is unknown, although many possibilities have been explored, including viruses, exposure to toxins in environment, family history and geography. Symptoms depend on the location and severity of involvement. It is usually diagnosed with a tissue biopsy, in addition to other testing, such as X-rays and blood studies. A biopsy of an involved site is necessary to make a definite diagnosis. LCH is a rare disease of the pediatric population, and it is about 4-5 per million [2] . Eosinophilic granuloma is a localized variant of LCH that usually affects children at 7-12 years age, especially boys. A single asympthomatic granulomatous lesion of the bone the most common manifestation. The cranium is most frequently affected. A spontaneous fracture or otitis media may be the first sign of disease. Skin and mucous membrane lesions are rare [1-2]. Lung, liver, spleen, bone marrow, lymph nodes, hypothalamic- pituitary region, gastrointestinal tract are among the organs that may be involved in LCH and should be examined in patients with suspect [2-3]. Case ReportWe present a case of a 7 year-old male with a history of redness in the eye and swelling of eyelid. He applied to an external center 9 days ago and have inpatient treatment with a preliminary diagnosis of sinusitis complication, preseptal cellulitis. According to external center’s epicrisis note, bilateral serous otitis media and postnasal purulent secretion were the inspection findings of ENT, ampicilin + sulbactam ® 4x0,5 gr IV were given along 6 days. The patient’s complaints were relatively decreased and he was discharged with a treatment of ampicilin + sulbactam 3x0,5 gr P.O ®. After three days of treatment the patient applied to us due to the relapse in complaints. When patient applied to us bilateral otoscopic examination was normal, purulent postnasal secretion was observed. Patient was hospitalized with a preliminary diagnosis of sinusitis complication, preseptal cellulitis. White blood count was 6700/mm3 (6000 - 11000/ mm3). C - reactive protein was 0,744 mg/dl (0 – 0,5 mg/dl). The left eyelid was slightly edematous and erythematous, bilateral conjunctiva and cornea were normal. Paranasal sinus computerized tomography (PNS-CT) scanning of the patient, mucosal thickening was noticed in both maxillary sinuses. At the inner wall of the frontal bone in the superiolateral of left globe, a destructive lesion in 15x 6 mm diameter was noticed. Swelling appearance was observed at left preseptal region soft tissue. Ophthalmologists recommended daily consultation.
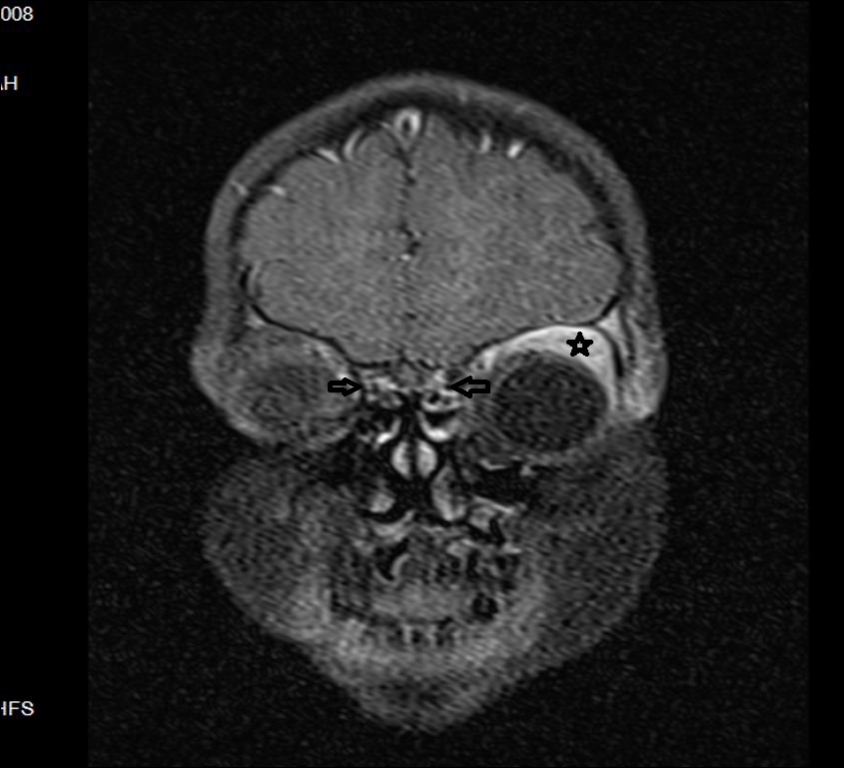
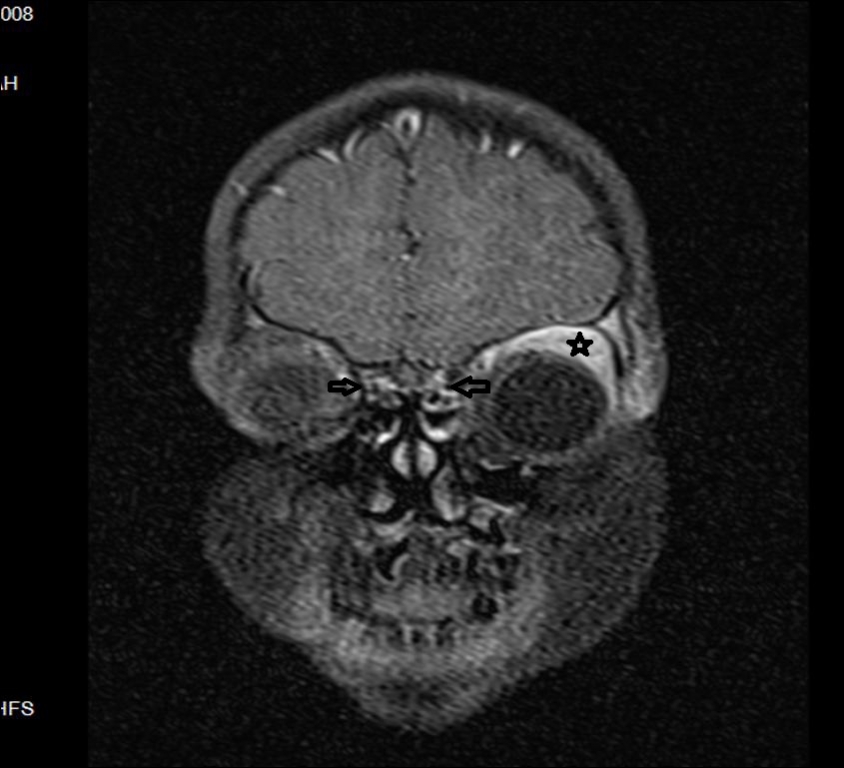
We cultured the aspiration material from nasal cavity but it remained sterile. We administrated empirical antibiotherapy for possible osteomyelitis with ceftriaxone ® 2x1gr and metronidazole ® 2x150mg but we did not achive any clinical response in 5th day of treatment. Vancomycin® (daily dosage is 40 mg/kg in 3 divided doses) was added to intravenous antibiotherapy with pediatric infectious disease specialists recommendation. He had nausea and vomiting during his inpatient followups, meningeal irritation findings were negative, and there was no stiff neck complaint. . In differential diagnose, soft tissue malignancy was also considered and Magnetic Resonance Imaging (MRI) with contrast revealed a lesion at superior area of left orbita in 17x9 mm diameter.
In T1 and T2 sequences contrast enhancement was noticed in frontal bone above the duramater in orbital gyrus level and soft tissue was edematous in preseptal area. His vision of the left eye, globe transactions, direct and indirect light reflexes, the intraocular pressure, front segment examination were normal. Bilateral posterior fundus optic disc and the macula were normal. Proptosis and enophtalmus was not detected. But the left eye edema and erythema were remained. Intravenous. Vancomycin therapy did not provide a meaningful improvement and a diagnostic operation was organized. The lateral left eyebrow incision was performed under general anesthesia. After we passed the subcutaneous skin, we reached the frontal bone, pathological area in soft tissue lesion was found to be localized in an area of the frontal bone erosion. We obtained an excisional biopsy and tissue culture. We continued intravenous Vancomycin® therapy postoperatively due to an osteomyelitis possibility. Tissue culture was sterile. In histopathologic examination the result was concordant with Langerhans Cell Histiyositosis (LCH). We made the diagnose of Langerhans Cell Histiocytosis and referred the patient to the Hematology/Oncology Clinic for treatment. DiscussionLangerhans cell histiocytosis, since it was defined for the first time, it was quite least understood as a disease by clinicians, patients and their families. In older children usually bone involvement with local swelling, pain and dysfunction is accompanied by localized form [4]. In children under the age of two, pain, restlessness, skin rash, weight loss, growth retardation, and general symptoms like fever is observed, organ dysfunction, accompanied by systemic form is seen [5-6]. Most commonly LCH was localized in bone, skin or lymph node, as a solitary lesion, however multiple lesions were also reported [7]. LCH may present with either systemic involvement with multiple organ involvement and dysfunction or solitary lesions. In literature, various organ involvement with different clinical findings were seen [8]. Bone and soft tissue are the most common sites of involvement, followed by, in order, skin, lymph, bone marrow, liver and spleen, and less commonly pulmonary and gastrointestinal system involvements are reported. Occasionally, thyroid gland, oral mucosa involvement and ovarian involvement is observed [9]. It would be enough to have conservative treatment approach in localized disease but in systemic disease, chemotherapy, radiotherapy or combined treatment could be needed. Etoposide, doxorubicin, vinblastin, prednisolone and cyclophosphamide are alternative agents of chemotherapy. This article describes atypical clinical findings of a pediatric patient with LCH. The reason to our delay in making the correct diagnose was the patient’s physical examination and radiological signs which were concordant with preseptal cellulitis. When we could not achieve any clinical response even after 5 days of wide spectrum antibiotherapy, this situation directed us to perform a to tissue biopsy for another diagnose like a osteomyelitis or a soft tissue sarcoma. We would like to emphasize with this report that, when a patient did not responded to antibiotherapy with a preliminary diagnose of sinusitis complication, preseptal cellulitis, LCH should also be kept in mind. AcknowledgementAuthor thanks Ayşe Şermin Filiz Acıpayam for her contributions. References
|
|||||||||
| Keywords : Langerhans hücreli histiyositoz , Preseptal selülit , Sinüzit komplikasyonu | |||||||||


|