

Authors
|
|||||||
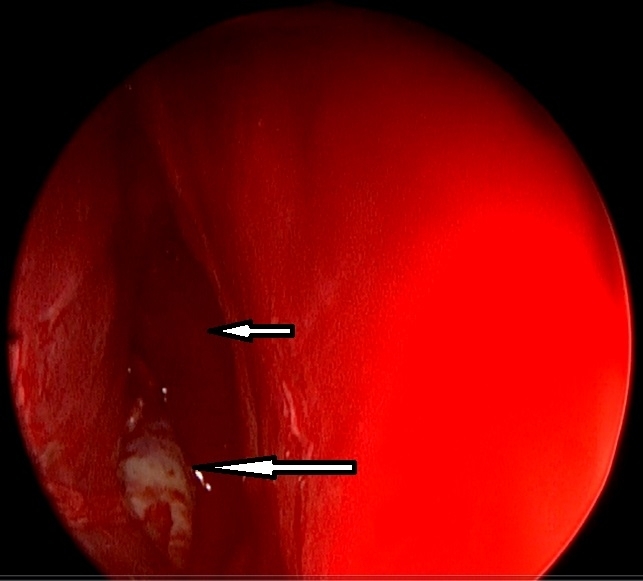
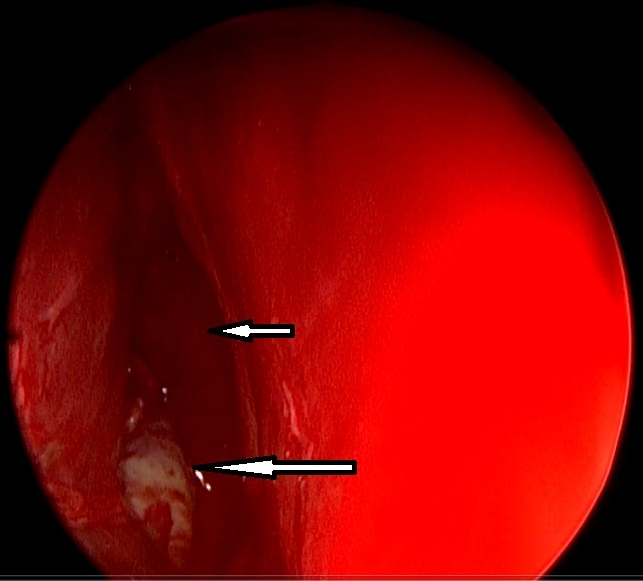
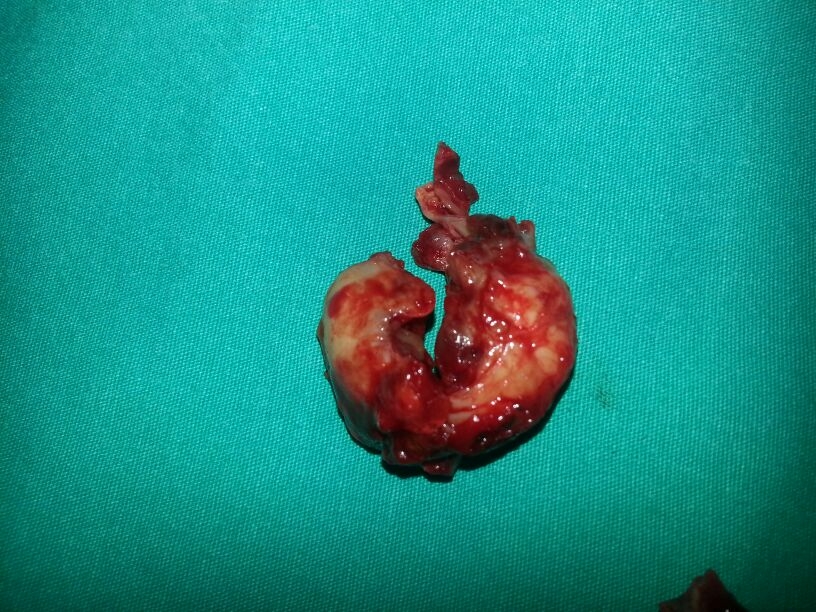
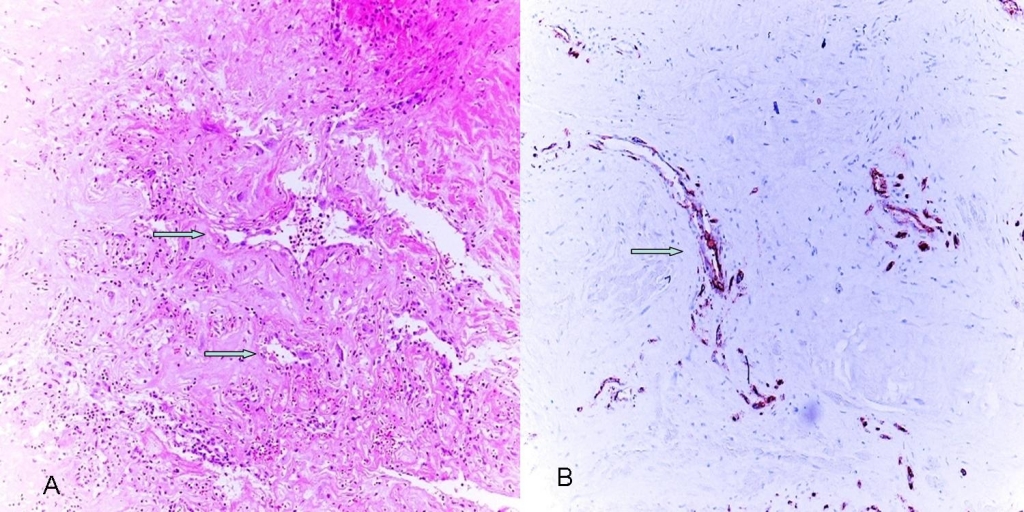
AbstractEpistaxis is a common symptom among patients attending to emergency department. Especially in unilateral intractable bleeding, tumors must be thought in differential diagnosis. Juvenile nasopharyngeal angiofibromas are benign but locally aggressive tumors of nasal cavity originating from sphenopalatine foramen region which are seen in adolescent male patients. Recently, extranasopharyngeal angiofibroma cases are rarely submitted in the literature. In this case report, we presented an extranasopharyngeal angiofibroma originating form right maxillary sinus in a 22 years old male patient with intractable bleeding who had no intranasal or nasopharyngeal mass. The case is discussed with the light of the current literature.IntroductionEstimated lifetime incidence of epistaxis is 60% and it is the commonest emergency for otorhinolaryngology [1,2]. Causes includes systemic reasons such as coagulopathies, renal failure, alcoholism, vascular anomalies and local reasons such as digital trauma, nasal septal deviation, neoplasms, chemical irritants. In unilateral epistaxis, tumors must be ruled out with imaging techniques and endoscopic evaluation [1]. Juvenile nasopharyngeal angiofibroma (JNA) is an uncommon, benign and locally aggressive tumor of nasopharynx which consists of 0,05-0,5% of all head and neck malignancies [3]. Classically, JNA manifests with recurrent epistaxis and nasal obstruction in an adolescent male patient [4]. Origin of the tumor is thought to be superior part of sphenopalatine foramen and posterior part of middle turbinate [3]. Recently there are case reports and series of angiofibromas originating from different sites in the head and neck region called as extranasopharyngeal angiofibromas(ENAs). Most common site of these tumors is maxillary sinus [5,6] In this case report , we discussed origin, sign and symptoms of ENAs and differences from classical JNAs with the light of current literature in a 22 years old male patient with a maxillary sinüs angiofibroma. Case Report22 years old otherwise healthy male patient admitted to emergency department with unceasing nose bleeding. He had no medical history such as trauma, coagulopathy or hypertension. In his physical examination, there was active anterior and posterior bleeding from right nasal cavity. Anterior rhinoscopy and endoscopical examination of the nasal cavities revealed right nasal septal deviation and active bleeding from posterior part of the deviation, the exact site of the bleeding couldn’t be seen. There was no nasopharyngeal or intranasal mass. Transnasal endoscopical surgery under general anesthesia is planned for controlling epistaxis. During surgery, after septoplasty bleeding from right maxillary sinüs was seen, uncinate process was medialized due to effect of intramaxillary mass. After uncinectomy, intramaxillary bleeding tumor was seen. (Figure 1) With functional endoscopic sinus surgery tumor was removed enbloc with anterior and posterior ethmoidectomy. (Figure 2) Postoperative histological examination of the tumor was well consistent with angiofibroma. (Figure 3) Postoperative period was uneventful and he had no more nose bleeding attacks for 1 year after surgery.
DiscussionJNA is an uncommon, benign and locally aggressive fibrovascular tumor of nasopharynx which consists of 0.05-0.5% of all head and neck malignancies. Exact reason of the tumor is unknown but since it is seen in adolescent(10-17 years) male patients and steroid hormone receptors( mostly androgens, rarely estrogen) are expressed in tumor cells, a hormonal theory is thought as an etiological factor [1,3,7]. Cases of recurrence after external testosterone treatment confirms hormonal theory [8] For maxillary angiofibromas unequal development of skull bones coupled with sex and age is suggested to be the cause [6]. Classically, JNA manifests with recurrent epistaxis and nasal obstruction in an adolescent male patient [4]. Although the name of the tumor is juvenile nasopharyngeal angiofibroma, exact origin of the tumor is superior part of sphenopalatine foramen and posterior part of middle turbinate, but nasopharynx can be invaded early during spread of the tumor [3,9]. Most serious complications of the tumor are intracranial spread and life threatening nose bleeding [7]. Routes of invasion of JNA are as follows: tumor firstly invades nasal cavity and nasopharynx then pterygomaxillary space. After erosion of bony structures it can invade to infratemporal fossa, orbita and middle cranial fossa [9]. Intracranial expansion is in 10-20% of cases. Classical radiological findings of JNA are nasopharyngeal mass with intense contrast agent enhancement, expansion in the pterygopalatine fossa, erosion in the pterygoid process of sphenoid bone. Holman-Miller sign (bulging of posterior wall of maxillary sinus anteriorly) is another characterized radiological sign [4,10]. Although origin of JNA is thought to be superior part of sphenopalatine foramen there are authors arguing that tumor is arising from pterygoid(vidian) canal [3]. While debates on origin of JNA are existing, recently, there are also case reports or series of angiofibromas originating from sites different than nasopharynx called as ENAs [5,6]. Although ENAs have same morphology with JNAs histologically, they can be classified as a different group since there are differences between ENA and JNA about clinical findings, origin site and epidemiological features [10]. In year 2000, Huang et al. published a review of 55 cases with ENAs which was the most broad case series about this issue in the English literature till this year [5]. After this, in year 2004 Wındfuhr et al. published a review of 65 cases with ENA [6]. Maxillary sinus was the most common site of origin (32% and 24,8%) in these series [5,6]. Our patient was also a maxillary sinus ENA. Mostly seen other sites of ENA are ethmoid sinuses, nasal cavity and nasal septum [6]. Other origin sites of ENA that can be seen in head and neck region are inferior and middle turbinate, lacrimal sac, piriform apertura, cheek and buccal mucosa, hard palate, larynx, tonsil, facial nerve, external ear and conjunctiva [6,10,11]. Angiofibroma of inferior turbinate can be seen primarily or after CO2 laser turbinoplasty [12,13]. There are fundamental differences between ENA and JNA. JNAs mostly manifest with epistaxis and nasal obstruction, symptoms of ENAs differ according to origin site. JNAs mostly originate from superior part of sphenopalatine foramen whereas ENAs most commonly originate from maxillary sinus. Average diagnostic age of JNA is 10-14 years whereas ENAs are mostly diagnosed at later ages such as 17-22 years old. Local recurrence rates of JNA differs between 6-27.5%. In ENA, extranasopharyngeal placement of the tumor enables total removal and recurrence is not seen. JNAs are mostly seen in adolescent male patients whereas ENAs are mostly seen in women. Hypervascularity of ENA is less than JNA [6,10]. In our case; age of the patient was 22 years old; an older age compared to classical JNA and intraoperatively there was less bleeding and hypervascularity without preoperative embolization compared to classical JNA. These findings are well compatible with differences between ENA and JNA described above. Although intranasal ENAs can show symptoms earlier due to less tumor space for growth, maxillary sinus ENAs can be insidious and can be diagnosed later [5]. Primary treatment of JNA is surgical excision after preoperative embolization. Small-medium sized tumors can be surgically excised endoscopically, whereas in large tumors of orbital or intracranial spread, external approach can be necessary [7]. For large and expansive tumors, radiotherapy, chemotherapy and hormonal treatment can be used [9]. In our case, since the patient was operated in an emergency situation, and there was no nasopharyngeal or intranasal mass preoperatively, embolization couldn’t be done. As a conclusion, for patients with unilateral recurrent nose bleeding, without nasopharyngeal or intranasal mass, maxillary sinus ENAs must also be thought in differential diagnosis. References
|
|||||||
| Keywords : Juvenil nazofarengeal anjiofibrom , Ekstranazofarengeal anjiofibrom , Epistaksis , Maksiller sinüs | |||||||
|