

Authors
|
|||||||||
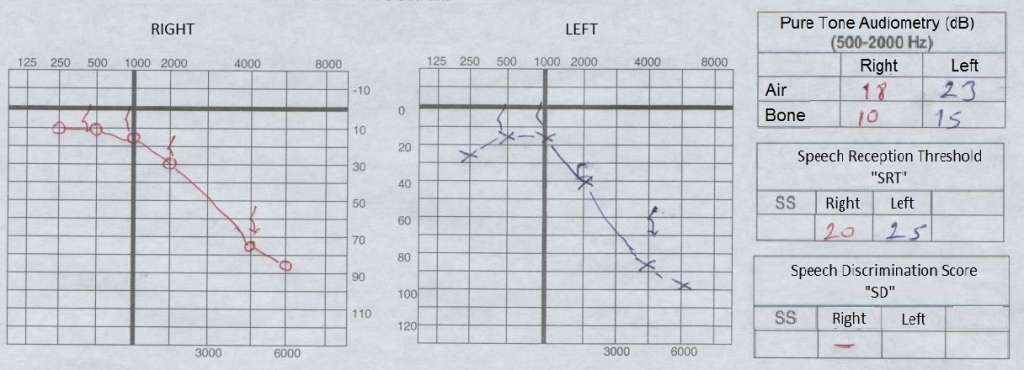
AbstractSudden hearing loss (SHL) is a sensorineural hearing loss (SNHL) occuring within last three days and at least in three consecutive frequencies worse than 30 dB. Hematological pathologies rarely takes place in etiology. In this case report, we present a patient who admitted to our Otolaryngology Department twice in two months with the complaint of sudden hearing loss in the right ear. In both times SHL has been diagnosed and the patient has been given medical treatment. Despite further investigation, there was no clue for the underlying diagnosis at the first time. At the second application of the patient, acute myeloid leukemia (AML) has been identified. We aimed to present first case in English literature: sudden hearing loss as a first sign of AML. For the management of recurrent SHL, hematological pathologies should be kept in mind and biochemical examination must be repeated for each application of patients.IntroductionAcute myeloid leukemia (AML) is a malignant disease group which is characterized by an increased rate of proliferation of the white cells compared to normal cells, decreased spontaneous apoptosis associated with the uncontrolled and clonal proliferation and bone marrow invasion by increasing rate of these cells [1]. In long-term follow-ups, survival in children are 40-60%, and 35% of all leukemia patients are lost depending on the disease and treatment toxicity. In recent years, by identifying high-risk patients and giving more intensive treatment to these groups, up to 90% event-free survival has been an increasing feature in high-risk patients as a similar rate in low-risk patients. Acute or chronic leukemias are rarely present with pathological findings [2]. Otological symptoms usually occurs due to bleeding, tumor infiltration, infection or hyperleukocytosis [3]. Since the strict diagnostic criteria of AML is to be above 30% of blast number in bone marrow aspiration and biopsy, bone marrow aspiration/biopsy is absolutely necessary. SHL is a sudden sensorineural hearing loss (SSNHL) occuring within last three days and at least in three consecutive frequencies worse than 30 dB [4]. The incidence have been reported 5 to 20 in 100.000 and it is usually one-sided [5]. In this case report we aimed to present the recurrent SHL in the way of diagnosis of AML, as well as the evaluation of the patient with SHL and to draw attention to the importance of the needs what to be done to uncover the possible etiology Case ReportA 80-year-old male who complains of tinnitus and hearing loss for two days in his right ear admitted to our department in January 2012. There was no sign of other possible causes such as pain, dizziness, dullness, trauma, exposure to loud noises and upper respiratory tract infection. In his otolaryngologic examination, the external ear canal was normal, a healthy tympanic membrane was observed and there was no otorrhea, cerumen or other pathological findings. Facial and other cranial nerve examination was normal. No spontaneous nystagmus was observed and fistula test was negative. In addition, other vestibular system and otolaryngologic system examination was normal as well. Weber tuning fork test lateralized left. In pure tone audiogram air/bone conduction at the right side was 55/48 dB and speech reception threshold (SRT) was 48%. Hearing level at the left side was normal (Figure-1).
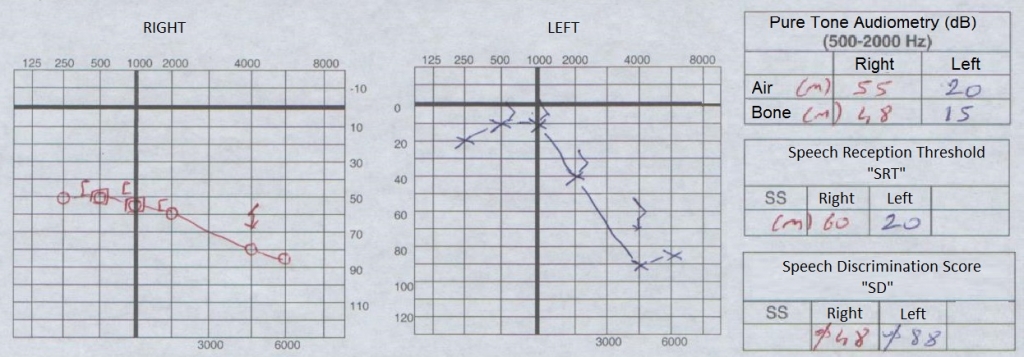
Tympanogram of type A curve was determined. The temporal/brain MRI and biochemical tests performed for etiology were normal. After explaining side effects and consultating other clinics regarding use of steroid, the patient was recieved the treatment of 1 mg/kg IV metilprednisolone (Prednol-l 40 Mg 1 Ampul, Mustafa Nevzat, Türkiye) and simultaneous hyperbaric oxygen therapy for seven days. The control pure tone audiogram at seventh day, air-bone conduction in the right side was 15/12 dB, SRT: 84%, and treatment was terminated (Figure-2).
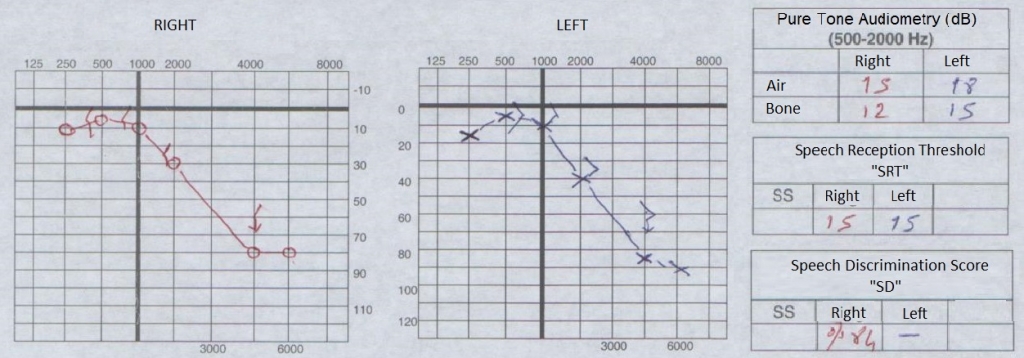
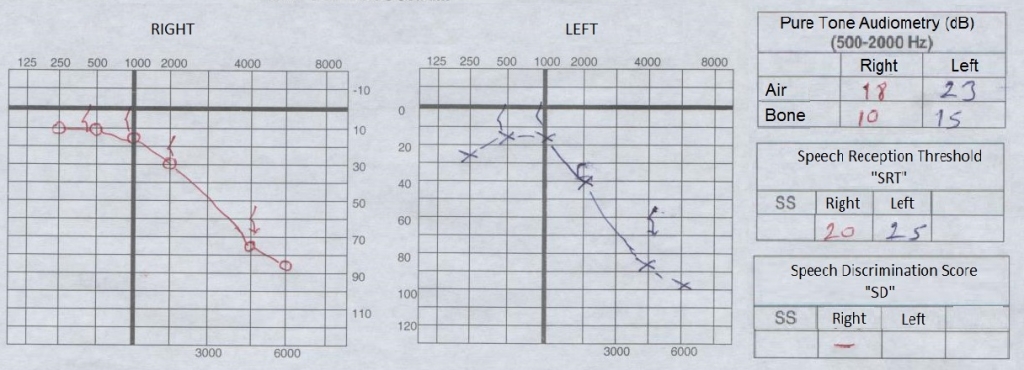
The patient's hearing loss in high frequencies was related with exposure to the chronic acoustic trauma as a result of being ex-military, which is confirmed by medical history and previous hearing tests. Two months later, the same patient presented with complaints of hearing loss and tinnitus in the right ear again and he is admitted to the clinic at the first day of hearing loss. There was no sign of other possible causes such as pain, dizziness, trauma, exposure to loud noises and upper respiratory tract infection as before. All other ENT and systemic examination was normal. In pure tone audiogram air/bone conduction at the right side was 40/40 dB and 18/18 dB at he left (Figure-3).
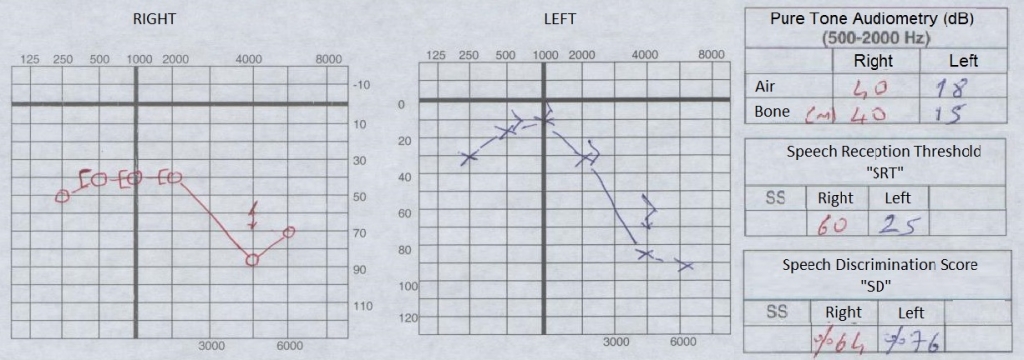
The patient was diagnosed right SHL again and 1 mg/kg IV dose of prednisolone and HBO therapy was administered concurrently for 5 days. The control pure tone audiogram showed air-bone conduction in the right side was 18/10 dB and treatment was terminated (Figure-4).
Taking into consideration the development of SHL in the same ear of the patient in the last 2 months, etiology for systemic pathologies was investigated. The blood tests were performed again and results were abnormal (hemoglobin: 11.9g/dL, thrombocyte: 81K/mm³, %monocytes:31.8%, %neutrophils:38.7%, white blood cells: 14.6K/mm³), so hematology consultation was performed. The peripheral blood smear made by the hematology clinic showed 36% blasts and the bone marrow biopsy was consistent with leukemic infiltration. As a result of flow cytometry, AML has been reported hence the expression of a molecules such as CD13, CD33, CD34, HLA DR, CD13+HLAR+, CD34+HLAR+. 5-azacytidine treatment was planned for the patient as 4-month-chemotherapy. Following this, 6 cycles of decitabine treatment was applied to the patient by hematology clinic. Written informed consent was obtained from the patient prior to redaction of this manuscript. DiscussionSHL is an otologic emergency that the etiology and treatment are still controversial. Approximately 95% of the rate observed only on one side [5]. Recurrence probability is lower from 1/100 [6]. Even though there is quite a long list of potential etiologic factors, 88% of all cases remain as idiopathic. Plenty of evidence as cause of idiopathic SHL shows viral infections, autoimmune mechanisms and vascular disorders. As a result, all these factors are believed to be effective in disrupting the cochlear microcirculation [7]. In the etiology of SHL, viral infections, trauma and idiopathic causes in addition with hematological diseases such as polycythemia vera, multiple myeloma, lymphoma and leukemia are included. These diseases are considered as causes of SHL in relation with vascular pathologies. SHL associated with acute lymphoblastic leukemia (ALL) or chronic myeloid leukemia (CML) are few in English literature [8], however SHL associated with AML has not been reported previously. Leukemia usually shows itself with some signs and symptoms such as fewer, bleeding manifestations, lymphadenopathy, ataxia, nystagmus, papilledema, blindness, headaches, dysarthria and coma. Otologic symptoms such as sudden hearing loss, vertigo, tinnitus, facial weakness and infection can be seen in leukemia patients ranged from 16-40% [8]. Sudden hearing loss among these, is very rare, moreover, hearing loss as the first sign of the disease is extremely rare. The first study on histopathological examination of hearing loss in patients with leukemia were published by Politzer [9]. Many published studies that evaluate the changes on the temporal bone in leukemia patients are available in literature. These changes are generally divided into three categories: 1-bleeding, 2-leukemic infiltration and 3-infection [3]. Inner ear bleeding between these three categories are considered as major etiological cause of sudden hearing loss [10]. The fibrosis and new bone formation detected in the temporal bone of these patient groups are long-term findings thought to be developed secondary to the bleeding [10]. Hyperviscosity syndrome developing due to hyperleucocytosis is also a possible cause of the hearing loss, but this syndrome usually occurs above 500000 WBC/mm3. Also, intracranial infiltration or vascular occlusion caused by a hematological malignancy may be the cause of sudden hearing loss in this patient group [8]. In our patient, there was a sudden hearing loss occuring 2 times in 2 months. In addition to the patient's hearing loss, tinnitus was present but did not have any symptoms or physical findings except for these two complaints. In both situation, sudden hearing loss was diagnosed and steroid treatment was given. Since recurrent sudden hearing loss is a rare condition and the patient is old, it was considered to be an underlying pathological condition that can cause this situation. Further biochemical and radiological examinations were repeated and the results revealed AML. In the treatment of SHL, vasodilators increasing local blood flow, volume expanders, anticoagulants, antivirals, hyperbaric oxygen therapy, steroids and intratympanic steroid treatment are available. So we began treatment with IV steroids. We observed that the patient's hearing threshold returned to normal limits in seven days. In conclusion, particularly in patients with recurrent SHL, possible etiological causes such as hyperviscosity, microthrombus, vasculitis or autoimmunity should be kept in mind. Biochemical and radiological examinations must be repeated for each application of patients. In the etiology, intracranial infiltration or vascular occlusion caused by a hematologic malignancy should be considered and additional symptoms must be questioned. Systematic assessment should be performed and other clinical consultations should be made. References
|
|||||||||
| Keywords : Ani işitme kaybı , akut myeloid lösemi , malignite. | |||||||||
|