

Authors
|
|||||||
AbstractLeishmaniasis is a parasitic disease group that is transmitted by the bite of infected female phlebotominic sand flies. It can be seen in 3 different forms such as cutaneous, mucocutaneous and visceral Leishmaniasis. Visceral leismaniasis (VL) can manifest in various clinical forms; causes malaise, weight loss and fever of unknown origin. In physical examination, pallor, hepatosplenomegaly and lymphadenopathy are common findings in the skin and mucous membranes. In this case report, we have been clinically clinically treated for 3 months with isolated cervical lymphadenopathy. A 34-year-old man was informed about the diagnosis and treatmentIntroductionLeishmaniasis describes a globally widespread group of parasitic diseases transmitted by the bite of infected female phlebotominic sandflies [1] . [ ]It can be seen in three different forms such as cutaneous, mucocutaneous and visceral leishmaniasis (VL) with or without lymph node involvement [2-3] . Visceral leishmaniasis (Kala-azar) is a protozoal infection that infects liver, spleen, and bone marrow macrophages, proliferating intracellularly [4]. It is known that VL is endemic in Aegean, Mediterranean and Central Anatolia regions in our country [4,5]. The disease is generally defined in three epidemiological forms according to the geographical regions it is seen all over the world. Mediterranean type: the reservoir is often dogs and the causative agent is L. Infantum . It usually causes disease in children. Indian type: reservoir is often humans and causative agent is L. Donovani. African type: reservoir is often rodent and is caused by a variety of factors. [[1] ] The disease can manifest in various clinical forms; it often causes weakness, weight loss and fever of unknown origin. On physical examination, pale skin and mucous membranes, hepatosplenomegaly and lymphadenopathy are common findings [4,6]. In laboratory examinations, severe and progressive chronic anemia, leukopenia with lymphocyte and monocyte dominance, thrombocytopenia, polyclonal hypergammaglobulinemia, hypoalbuminemia, and occasionally liver function tests can be detected. Isolated lymphadenopathy is a rare condition [6]. In this study, an unusual case of visceral leishmaniasis with isolated cervical lymphadenopathy in an immunocompetent host is presented. Case Report34 year old male patient applied to our outpatient clinic on August 2019 with a lymphadenopathy clinic of two cm in the right level three region, which has been present for three months. In his anamnesis, he has no other disease, with cardiac arrhythmia as an additional disease. There is no history of fly bite, travel, wandering, or suspected sexual contact. In his examination, there was a palpable, painless lymph node of two cm in the right level two-three region. No additional pathological finding was detected in the physical examination. No abnormalities were found in laboratory blood tests.(Hb:14.7, WBC:5.3 , PLT:182000 , CRP:0.3 , ALT:41 , AST:32 , GGT:26 ) In order to evaluate it in terms of tularemia and other granulomatous diseases, the patient was consulted for infectious diseases. Tularemia blood was sent to the public health laboratory. However, tularemia serology was negative. In the desired neck ultrasonography of the patient; in the right level three, cortical asymmetry and fatty hilus was selected, and a spherical lymph node with a size of approximately 15 * 17 mm . Vascularization from the hilus was observed with RDUS examination. Fine needle aspiration biopsy performed with the consent of the patient; "There are cells in smear preparates, some of which are atypical and whose nature cannot be fully evaluated." it resulted in the form. After obtaining verbal and written informed consent from the patient, the operation was performed under general anesthesia for the excision of the mass for further diagnosis and treatment. It was sent for frozen examination during the operation. It was reported that epithelial malignancy was negative, but lymphoid neoplasia could not be ruled out. There was no problem in the operative and postoperative period. Histopathological diagnosis; It was reported as being compatible with leishmania infection in the lymph node (Figure 1).
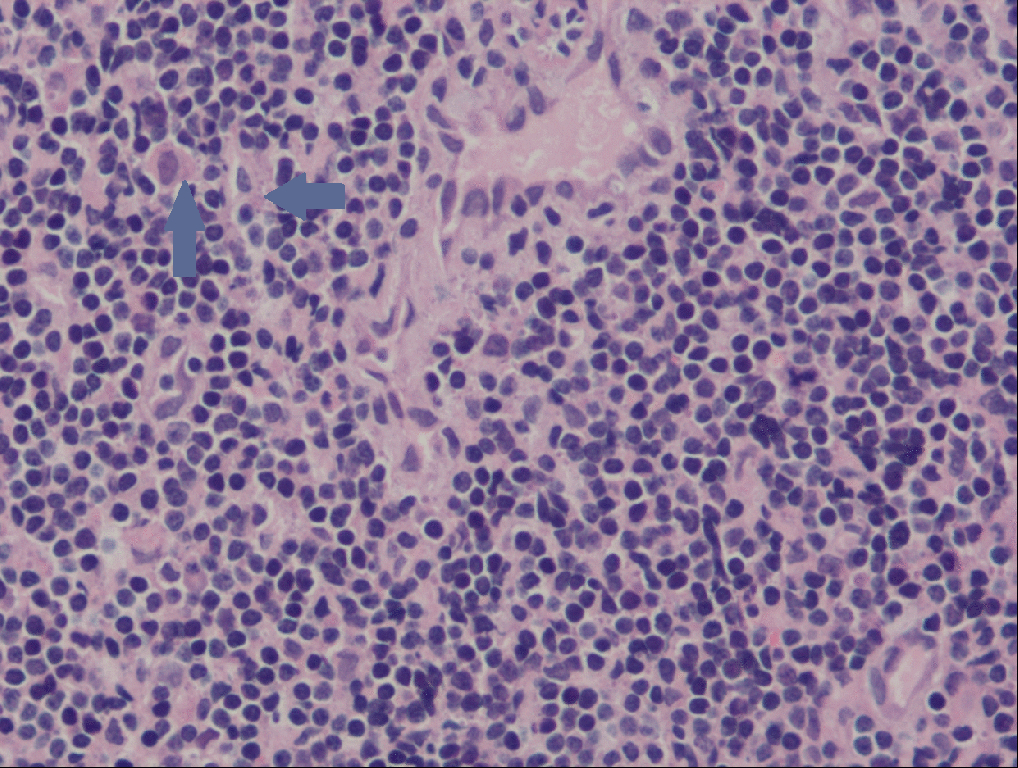
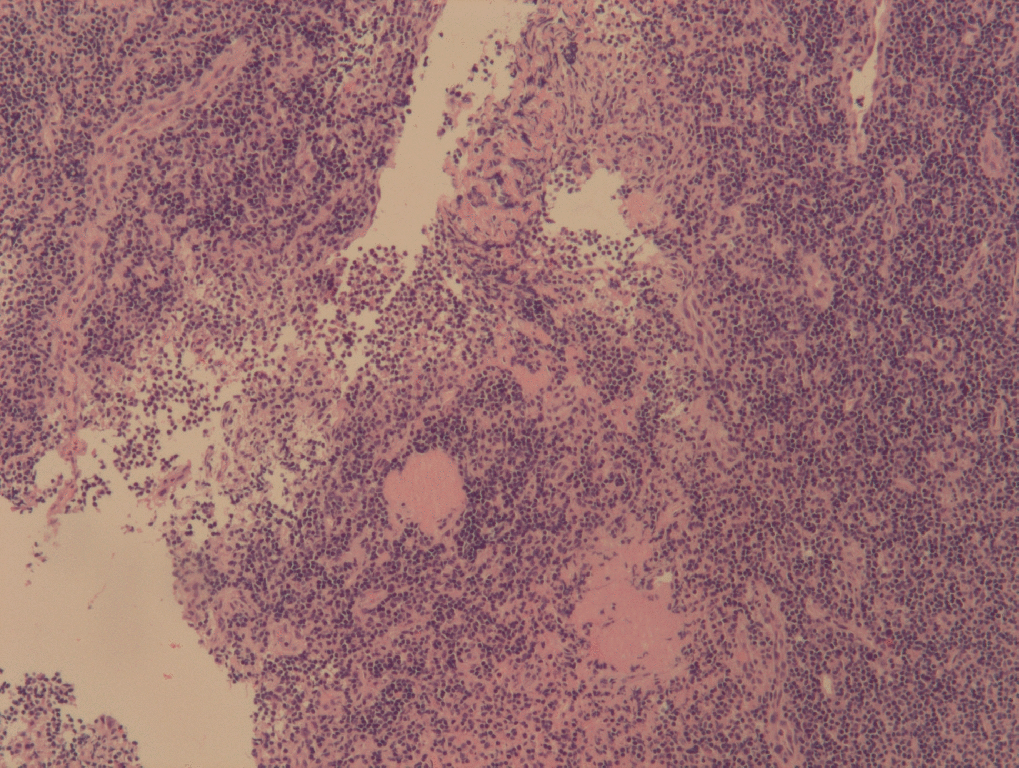
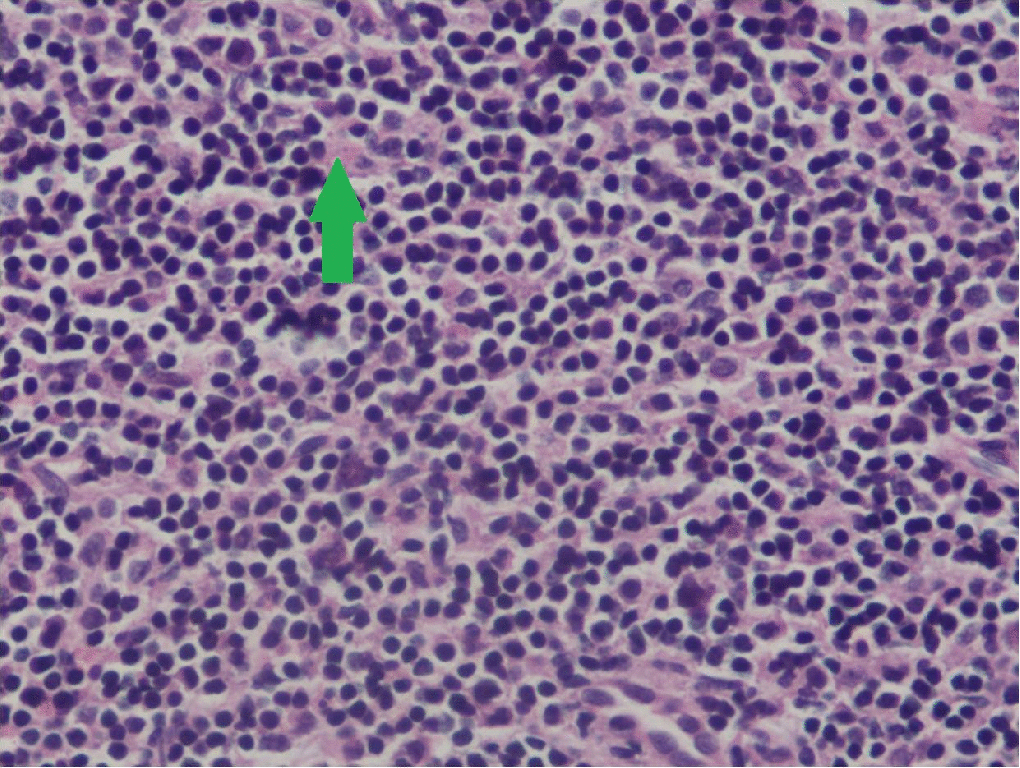
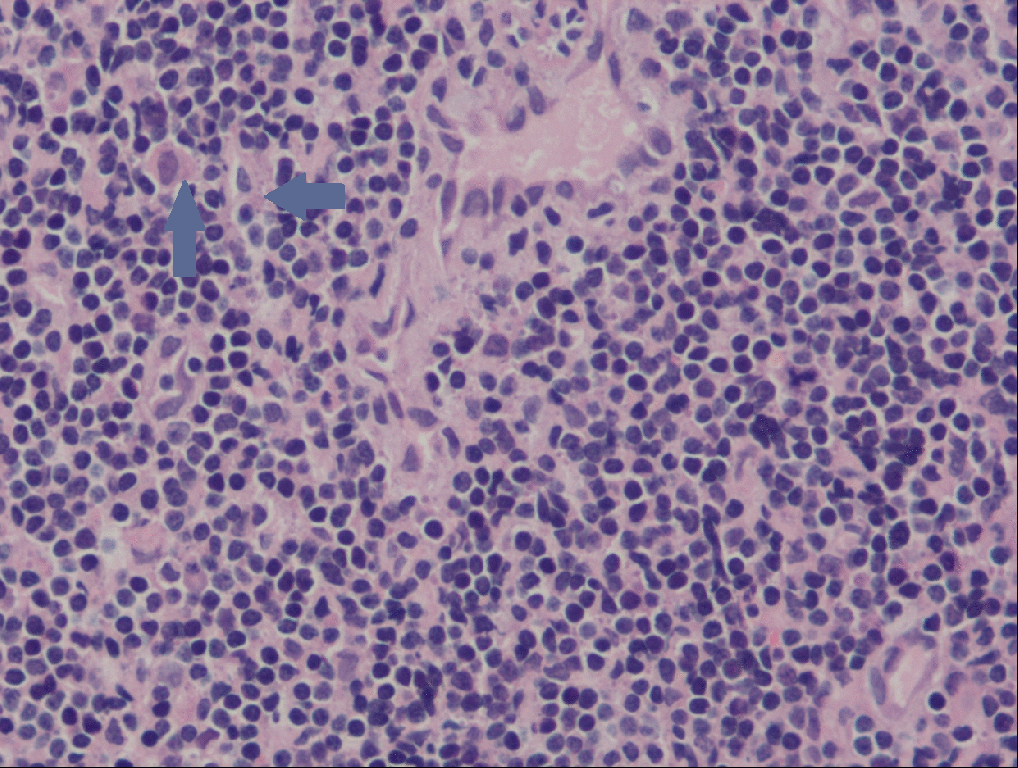
Microscopy: A picture of lymphadenitis with reactive lymphoid changes is observed in sections of the operation material whose presence of epithelial neoplasia was ruled out with intraopertative consultation. The presence of eosinophilic, oval-round structures smaller than lymphocytes at high magnification was noted in the evaluations made on the operation material, all of which were processed and examined with serial sections. These globular structures are thought to be compatible with leishmania in the foreground. Lymphadenitis table showing reactive changes (H&E, 100x) (Figure 1). Leishmania infantum amastigote form (green and blue arrows; H&E, 400x) (Figures 2 and 3)
The patient was reconstructed for Infectious diseases with his results. Since no glucantime treatment was available, fluconazole 1 * 200 mg po 6-week treatment was planned as an alternative treatment. No additional symptoms were observed in the subsequent follow-up of the patient. DiscussionCutaneous leishmaniasis, although seen as endemic in eastern Turkey, more visceral leishmaniasis Aegean, Mediterranean and Central Anatolia regions is seen in children under 15 years of age and male gender were found at greater risk. [7-8] Our case is 34 years old male and does not live in rural areas. Since visceral leismaniasis affects the reticuloendothelial system, it causes a series of systemic symptoms. Cardinal symptoms of the disease include fever, weakness, weight loss, hepatosplenomegaly, and lymphadenopathy, which starts subfebrile first and then rises twice a day within 1-2 weeks. [9] Lymphadenopathy can be seen with all types of leismania. However, localized lymphadenopathy without any and there was no weight loss in his anamnesis, hepatosplenomegaly cutaneous or systemic manifestations is rarely a finding of leishmaniasis. [10] Our case was immunocompetent was not found in the examination performed by the internal medicine department, the vitals were followed up stably. Only in the right cervical region, there was a two cm palpable, painless lymph node in the level two- three region. It is interesting that the pathology revealed leishmania in an isolated LAP case, and such cases are not rarely found in the literature. A definitive diagnosis is made by producing the organism in culture or showing amastigotes in tissues. Since our patient had isolated lymphadenopathy, an excisional biopsy of the lymph node was planned and sent for pathological examination. The diagnosis of leismania was confirmed by seeing amastigotes in the pathological examination. Although liver biopsy and spleen puncture are valuable diagnostic methods, both carry the risk of life-threatening hemorrhage. [11] Since our patient did not have hepatosplenomegaly, such procedures were not performed. Enzyme Linked Immunosorbent Assay (ELISA) and IFAT are reliable diagnostic methods among serological diagnostic methods. IFAT is a commonly used method for diagnosing leishmania. There are cases in the literature with asymptomatic IFAT (+) detection. [12] Serological methods may help diagnosis in situations where invasive procedure is not appropriate. In our case, since there was no contraindication in the patient and lymphoid malignancy could not be ruled out in the patient, total excision of the mass was planned by surgical method. Kumar et al. reported that localized leismaial lymphadenopathy is a condition that can be cured without treatment in an immunocompetent patient. [13] Since glucantime treatment could not be found in our case, fluconazole treatment was started for infectious diseases and was given 1 * 200 mg for 6 weeks. No additional symptoms or signs were observed in the patient's follow-up for 1 year. Conclusion As a result , isolated lymphadenopathy is a rare clinical manifestation of leismaniasis. Leismaniasis is one of the important diseases that should be kept in mind in the differential diagnosis of isolated lymphadenopathy in endemic countries. References
|
|||||||
| Keywords : leismaniazis , lenfadenopati , nadir | |||||||
|