

Authors
|
|||||
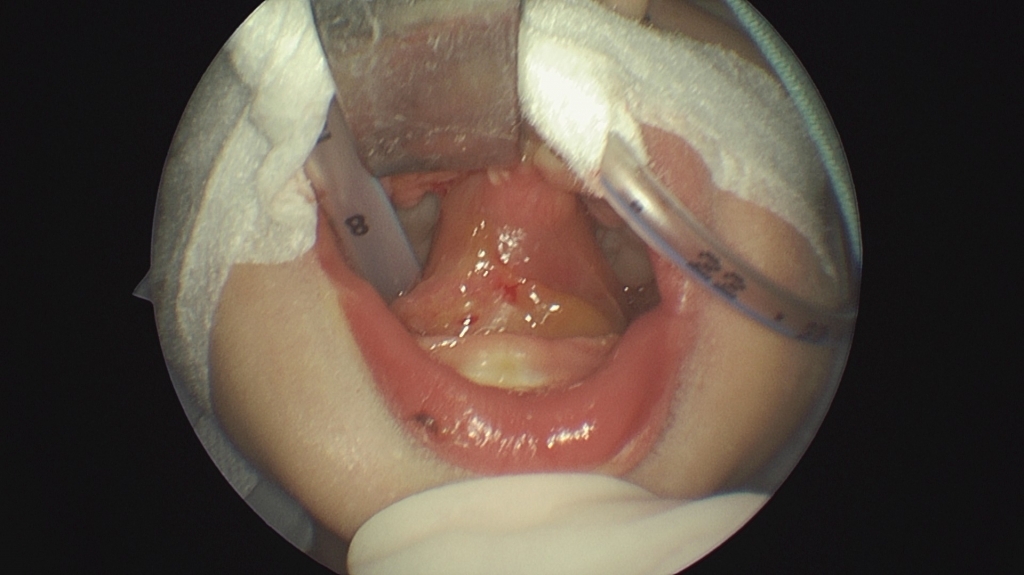
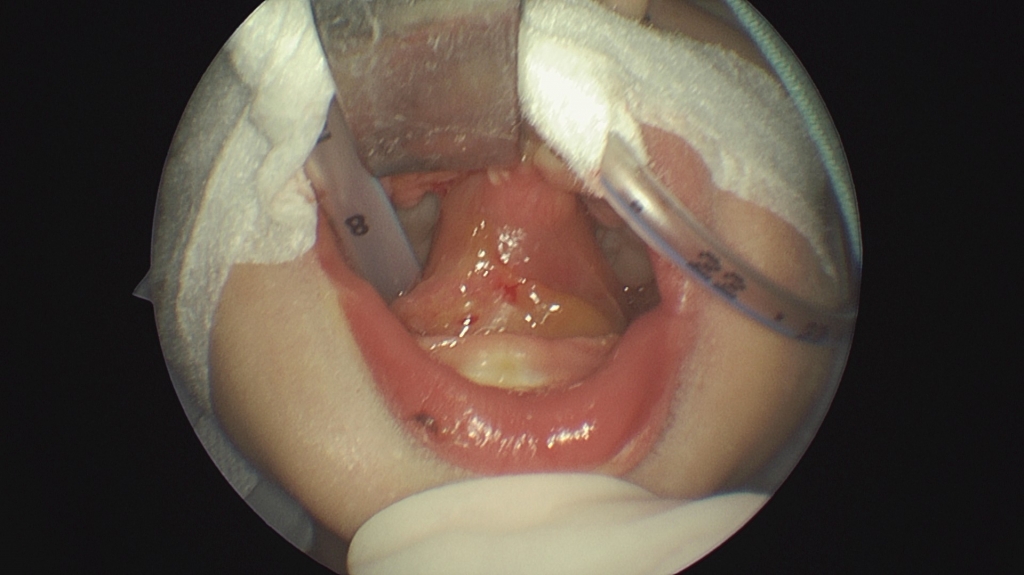
AbstractIntraoral synechiae is a rare anomaly. In many patients, intraoral synechiae is accompanied by cleft palate. The biggest problem associated with intraoral synechiae is restricted mouth opening that causes airway and nutritional problems. In neonates, congenital intraoral synechiae may be accompanied by other anomalies that may require emergency tracheal intubation. In neonates with intraoral and/or laryngeal abnormalities, performing nasopharyngeal examination with flexible endoscopy before intubation can provide an idea about intubation. In this report, we present a neonate with tongue-palate fusion with cleft palate and we aimed to discuss the emergency intubation procedure.IntroductionIntraoral synechiae refer to abnormal fibrous or soft tissue adhesions between intraoral structures. Patients with intraoral synechiae are highly rare. In contrast, epithelial synechiae are highly frequent and bone structure synechiae are relatively less common [1]. In the majority of patients, these synechiae are accompanied by a cleft palate. Intraoral synechiae typically involve the tongue, maxilla, mandible, floor of the mouth, and hard and/or soft palate. Glossopalatal ankylosis, also known as anterior midline glossopalatal ankylosis, is synechiae between the tongue and the margins of the palate or maxillary alveoli [2]. In the development of normal palatogenesis during the seventh week of embryologenesis, the palatal shelves are separated and displaced downwardly by the tongue. In the ninth week of development, the tongue is pulled down and protrudes from the oral cavity, thereby causing the palatal shelves to be elevated to the midline and to fuse with the primary palate and then with each other [3]. Normal palatogenesis may be impaired due to the presence of cleft palate caused by intraoral synechiae or the inability of the tongue to move downwards. To date, numerous pathogeneses have been proposed for intraoral fibrous bands. Additionally, persistence of the buccopharyngeal membrane has been proposed as a potential cause of intraoral fibrous bands and it has been suggested that buccopharyngeal membrane remnants could be the cause of posterior bands between the tongue and palate [2]. Intraoral synechiae may occur as a single entity or may be associated with other congenital anomalies or syndromes such as Van der Woude syndrome (VWS), popliteal pterygium syndrome (PPS), cleft palate-lateral synechia syndrome (CPLS), and oromandibular limb hypogenesis syndromes (OLHS) [4]. The fusion process of the palate during the 7[th] and 8[th] week of gestation may be disrupted by genetic, teratogenic, or mechanical factors [5]. This disruption, in turn, leads to abnormal fusion between the upper and lower gums, palate, and floor of the mouth, resulting in intraoral fibrous bands and cleft palate [2]. In such cases, the major problem is insufficient mouth opening for feeding, and intubation can be difficult since it is performed without viewing the larynx and without palpation. ensuring airway safety to eliminate respiratory distress in neonates with intraoral synechiae is of paramount importance. Accordingly, the goal of surgery is to remove adhesion to allow a normal mouth opening for airway passage, nutrition, and normal mouth development [6]. In case of feeding difficulties, a nasogastric tube may be placed. Moreover, utmost care is required while performing intubation for anesthesia induction [7]. Intraoral fibrous bands often have a good prognosis. To date, only one case of recurrent oral synechiae despite treatment has been reported, which could be due to the wide area of adhesion to the buccal and oral membrane [8]. In this report, we present a neonate with tongue-palate fusion with cleft palate and we aimed to discuss the emergency intubation procedure. Case ReportA female term newborn infant was brought to our pediatric clinic by her family two hours after birth due to intraoral synechiae that caused restricted mouth opening and difficult oral feeding. The mother and father were aged 26 and 29 years, respectively. It was the mother’s first pregnancy and she had no maternal disease or teratogen exposure during pregnancy. The infant was born vaginally in a hospital environment. Family history was negative for oropharyngeal anomalies or joint pterygia/contractures. In initial examination, synechiae were detected between the tongue and the hard palate (Figure 1) and the anomalies were limited to the mouth and oropharynx.
The infant also had bowel necrosis and thus was planned for surgery for both bowel necrosis and intraoral synechiae in the same session in order to prevent complications that could arise from the lack of oral nutrition in the early period after birth. Although the patient was stable, flexible nasal endoscopy and tracheostomy preparation were performed before blind nasoendotracheal intubation attempt due to restricted mouth opening and suspicion of other possible upper respiratory tract anomalies. Before performing endotracheal intubation in the operating room, upper airway examination was performed with flexible nasal endoscopy. In this examination, no additional anomalies were detected in the nasal passage, nasopharynx, or larynx, and no anomaly that could prevent airway intubation was detected. Anesthesia was induced with inhalation of sevoflurane (1-2%), without using any myorelaxants. Blind nasoendotracheal intubation was achieved in the first attempt. Under general anesthesia, the synechiae between the tongue and the hard palate was excised and the tongue and hard palate were separated (Video 1).
Adequate mouth opening was achieved. A detailed oropharyngeal examination was performed. The cleft palate was exposed after the release of the tongue. There was no desaturation during the intervention. No postoperative complications were observed. The repair of the cleft palate was postponed to a later time. The family was trained on how to feed the infant. In the latter stages of the operation, the patient was operated on by pediatric surgeons. During the operation, necrotic areas and multiple perforations were observed in the region extending from the distal part of the transverse colon to the sigmoid colon and in the sigmoid colon and the rectum. Necrotic areas were excised and colostomy was performed. The infant was followed up clinically in the neonatal intensive care unit. A standard chromosome analysis showed a normal 46,XX karyotype and no deletion, duplication, or rearrangement in the chromosomes. The patient died of sepsis caused by bowel necrosis. DiscussionIntraoral synechiae are rare and, as seen in our patient, are often associated with cleft palate. Almost 70% of synechiae cases present with a cleft lip and/or palate and the remaining 30% have other congenital anomalies. Synechiae can occur between different structures of the oral cavity. Moreover, although synechiae may coexist with other craniofacial abnormalities, intraoral synechiae are mostly accompanied by cleft palate [9]. The precise etiopathogenesis of intraoral synechiae remains unknown and there are several theories proposed by researchers, which primarily focus on buccopharyngeal membrane remnants, subglossopalatal membrane development, and abnormal fusion of immediately adjacent structures [2, 5]. On the other hand, although the presence of a total or partial buccopharyngeal membrane is rare, it has been reported in several cases in the literature [10]. Gartlan et al. [2] proposed similar mechanisms for the formation of a subglossopalatal membrane and glossopalatal ankylosis. The subglossopalatal membrane is a membrane that adheres to the margins of the cleft or soft palate superiorly and to the floor of the mouth inferiorly, and the glossopalatal ankylosis is congenital adhesions between the tongue and palate. In both conditions, pathological membranes prevent the downward and forward movement of the tongue. As a result, the tongue is positioned between the palatal layers superiorly and inferiorly, thus preventing the fusion of the palatal layers in the midline, which may be the primary reason as to why cleft palate is most commonly accompanied by intraoral synechiae [2]. During this embryogenesis process, genetic, teratogenic or mechanical factors can lead to an abnormal attachment between intraoral structures [2, 11]. In addition to these two theories, there are other reported factors that should be considered in the etiology of intraoral synechiae, such as prolonged contact between the epithelial lining of the oral cavity and the floor of the mouth, early fusion of the gingiva, and environmental factors (use of meclizine and high-dose vitamin A) [12]. In neonates with poor oral intake, intravenous glucose therapy can be administered to prevent hypoglycemia. However, this therapy may delay their sucking reflex. Additionally, when central venous catheterization is impossible and thus intravenous fluid therapy cannot be performed, the infant should be operated on urgently, predominantly to provide adequate mouth opening required for oral nutrition [13]. This can be achieved by separating the synechiae with a simple incision. In such patients, intubation can be performed by blind nasoendotracheal intubation or fiberoptic bronchoscopy, but the physician should also be prepared for tracheotomy before anesthesia. Additionally, the airway passage should be secured by examining the nasal passages, nasopharynx, and larynx using flexible nasal endoscopy before intubation [14]. Subsequently, intubation can be achieved in the first attempt. Another issue is the choice of anesthetic technique for these patients. Avoidance of muscle relaxants before endotracheal intubation will enable the patient to wake up in a shorter time and to perform a safer surgical intervention in undesirable conditions during a possible intubation difficulty or tracheotomy [13, 14]. Conclusion Congenital intraoral fibrous bands are extremely rare and can lead to functional deficiencies, particularly in terms of airway passage and nutrition. These bands are commonly accompanied by abnormalities. Although cleft palate is an extremely rare anomaly, it is the most common anomaly accompanying synechiae. Early treatment provides favorable results. Associated anomalies such as cleft lip and palate are treated with routine protocols and regular follow-ups. In addition, performing flexible nasal endoscopy before blind nasal intubation can be highly beneficial for physicians in such cases. References
|
|||||
| Keywords : Doğumsal anomaliler , Yarık damak lateral sineşi sendromu , Ağız içi sineşi , Hava yolu tıkanıklığı. | |||||

|