

|
|||||
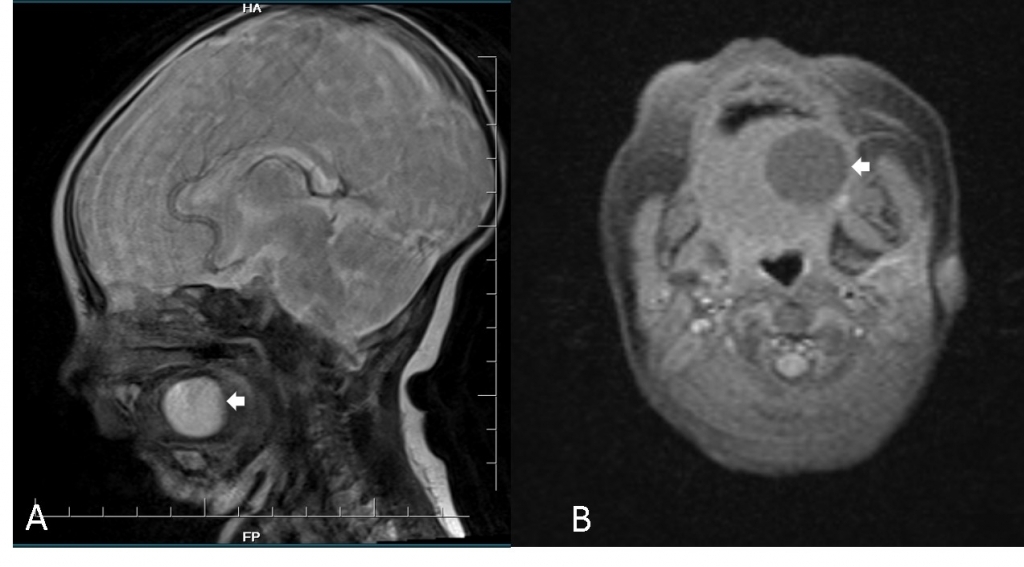
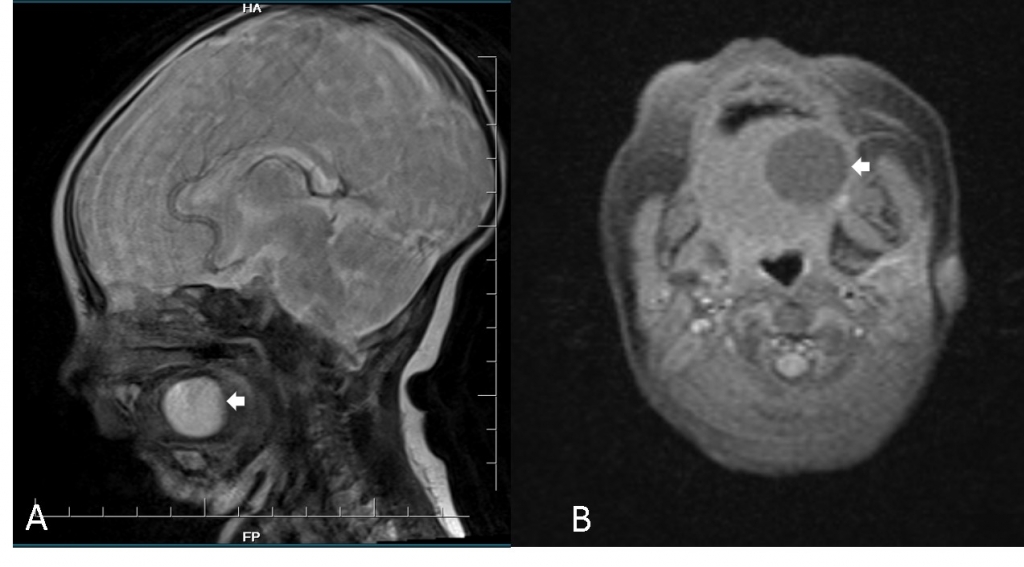
AbstractMucoceles are common cystic salivary gland lesions. The commonest site is the lower lip but can affect any part of the oral mucosa and the involvement of the tongue is rare. Large oral mucoceles may cause breastfeeding problems by restricting tongue movement. Here we report a 35-day-old infant girl who presented with tongue swelling and feeding diffuculty. Mucocele diagnosis was confirmed by Magnetic Resonans images and surgical resection was performed. The histopathologic evaluation was consistent with minor salivary gland mucocele. Tongue mucoceles can be a rare cause of sucking problems. Recurrence can be prevented by complete removal of the mucocele.IntroductionMucoceles are the most common benign cystic lesions of the oral cavity [1]. Mucoceles caused by occlusion of major or minor salivary glands. They are most frequently located in the lower lip in the mouth and are most common in the second decade of life [2]. Tongue mucoceles are rare and are most common on the ventral side of the tongue. Mucoceles can also be seen in the dorsal, lateral and tongue base [3,4]. Large mucoceles of the tongue may cause breastfeeding problems by restricting tongue movement.5 We report an infant girl with breastfeeding problems caused by a large cystic lesion of the tongue. Case ReportA 35-day-old infant girl presented with feeding difficulty and swelling of the tongue for 1 week. Her medical history was unremarkable. There was no history of oral trauma, oral surgery, foreign bodies, or medical illness. An examination of her tongue revealed a non-tenderness, superficial, protruding, fluctuant, soft on palpation, and approximately 2x2 cm in diameter on the left lateral side of the tongue. No ulceration was observed on the overlying mucosa.There were no palpable masses on her neck. Magnetic Resonance Imaging (MRI) showed a cystic lesion on the left lateral surface of the tongue in hyposignal T1 and hypersignal T2. The cyst measured 19x17 mm in a diamater. There was no gadolinium enhancement (Figure 1A,B).
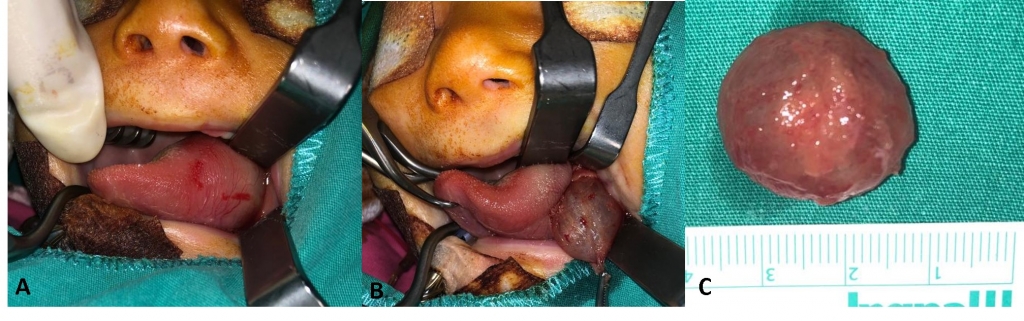
Histopathologic examination of the cyst showed a submucosal cystic lesion with a squamous wall and mucous glands. There was no mitotic activity, nuclear pleomorphism or necrosis. Histopathological examination confirmed the diagnosis of the tongue mucocele, and clinical evaluation at 2-year follow-up demonstrated no evidence of cyst recurrence. DiscussionMucocele is a common benign lesion of oral mucosa that ocur due to obstruction of the duct of minor or accessory salivary gland, causing mucous accumulation, especially in young individuals. It usually appears as a solitary painless swelling, fluctuant, and imparts transparent to bluish hue to the lesion. The most common site of occurrence of mucoceles is the lower lip, followed by tongue, buccal mucosa, palate, and retromolar area [6,7]. Tongue mucoceles can be congenital or acquired. Acquired mucoceles can be caused by physical trauma such as biting or tearing; Therefore, the lower lip is the common site of these cysts. However, they can also result from a blockage in the salivary duct caused by a sialolith or a mucus plug [4]. In our case, the absence of congenital complaints suggests that the acquired mucocele or small-sized congenital mucocele, which was not noticed before, may have enlarged. The clinical symptoms of tongue mucoceles vary depending on the size and location of the lesion. Small mucoceles can be asymptomatic. Speech, chewing and swallowing disorders can be seen due to large mucoceles [4]. Radiological imaging is necessary when diagnosis is unclear. Magnetic resonans imaging (MRI)is superior to computed tomograpy scans for oral cysts due to provide excellent soft tissue detail and distinguish the content of cyst. MRI of the mucoceles usually show high signal intensity on T2-weighted images and low signal intensity on T1-weight images [3,4]. The differantial diagnosis of tongue mucocele includes other etiologic factors causing tongue swelling such as, abscess, lipoma, fibroma, pyogenic granuloma, hemangioma, lymphangioma, salivary neoplasms, recurrent herpes, mucous pemphigoid, hematoma and squamous papilloma [8,9]. Other than these, ectopic tongue localized thyroid should be kept in mind in the differential diagnosis [10]. The treatment of mucocele is surgical. When possible, it is beneficial to identify and remove the minör salivary glands associated with the mucocele to reduce the rate of recurrence [8]. Laser or cryosurgery ablation of the mucocele, marsupialization and intralesional steroid injection are other treatment options [2]. To make histopathological distinction from other cystic masses, it is important to subtract total instead of marsupialization [11]. Needle drainage and simple incision are not recommended for treatment due to the risk of recurrence. It has been reported in cases that resolved spontaneously [2]. ConclusionIn conclusion, mucoceles of the tongue are rare in infants. Although it is most common on the ventral side of the tongue, it can also be located on the lateral surface of tongue. Depending on its size and location, it can cause breastfeedig problems. Complete removal of the mucocele is recommended to prevent recurrence. References
|
|||||
| Keywords : Mukosel , infant , beslenme zorluğu | |||||
|