Abstract
Arachnoid Pacchioni’s Granulations are little bulges of the arachnoid mater into the cerebral sinuses. They are mostly found in the transverse or superior sagittal sinuses. Arachnoid Pacchioni’s Granulations provide passive filtration of cerebrospinal fluid from the subarachnoid space. Their normal size is a few millimeters, but their size increases with age. They are usually asymptomatic, but rarely can cause venous hypertension. They also can be misdiagnosed as cerebral sinus thrombosis on computed tomography and magnetic resonance imaging. Cerebral sinus thrombosis can occur with nonspecific symptoms such as acute unilateral hearing loss. We present a rare case that applied to our clinic with sudden sensorineural hearing loss and incidental Arachnoid Pacchioni’s Granulation. In this case, we will discuss the distinction between Arachnoid Pacchioni Granulation and sinus vein thrombosis in the light of the literature.
Introduction
Arachnoid granulations (AGs), also known as Pacchioni’s granulations, are little bulges of the arachnoid mater into the cerebral sinuses that extend from the dura defects. AGs provide passive filtration of cerebrospinal fluid (CSF) from the subarachnoid space. Their normal size is a few millimeters, but their size increases with age [1,2]. They are mostly found in the transverse or superior sagittal sinuses [3]. They are generally asymptomatic, but rarely can cause venous hypertension due to partial sinus obstruction [4]. Giant arachnoid granulations can be misdiagnosed as cerebral sinus thrombosis [5]. In this article, we aimed to present a case who presented to our clinic with sudden sensorineural hearing loss (SSNHL) and incidental giant arachnoid granulation in order to emphasize the importance of differential diagnosis between Pacchioni’s granulations and cerebral sinus thrombosis.
Case Report
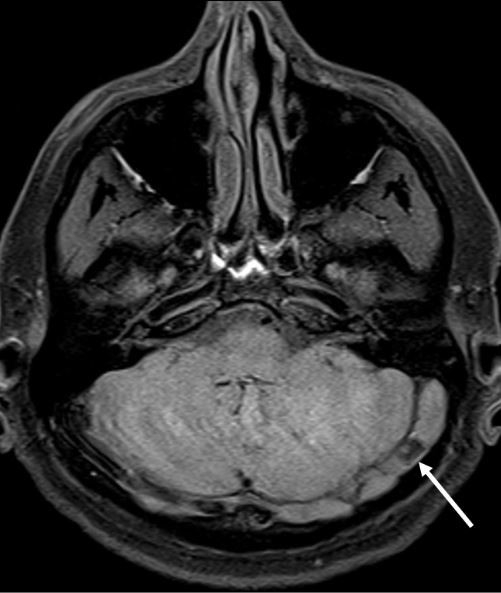
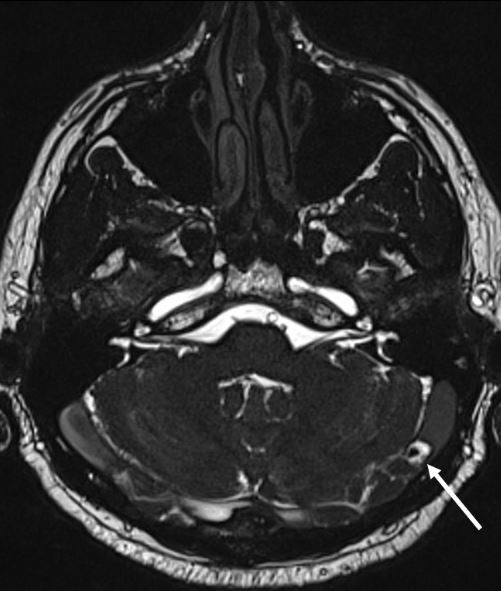
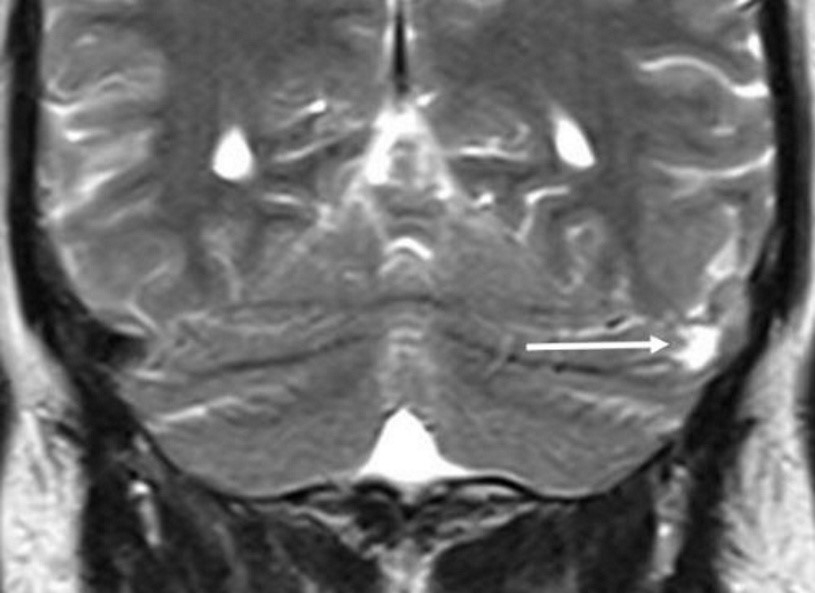
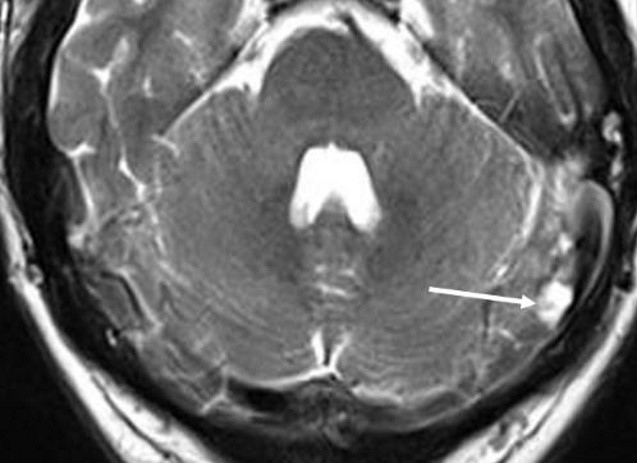
A 35-year-old man was admitted to our clinic with sudden hearing loss on his left side. The patient's hearing impairment, high frequency tinnitus, and left-sided headache had started 2 days before admission. Routine physical examination, complete blood count and routine blood biochemistry were normal. After admission to hospital, standard audiologic tests were performed (pure tone audiometry, tympanometry) and left‐sided SSNHL was observed. The audiogram showed severe sensorineural hearing loss on the left-side (pure tone average for 500 Hz, 1000 Hz, 2000 Hz and 4000 Hz, right/left: 59/110 dB; percentage of speech discrimination, right/left: 76/0). The patient had a history of bilateral sensorineural hearing loss for 2 years (pure tone average for 500 Hz, 1000 Hz, 2000 Hz and 4000 Hz, right/left: 55/58 dB; percentage of speech discrimination, right/left: 76/72). There was no other disease in the patient's medical history. 3D FLAIR Enhanced with Gadolinium internal auditory and inner ear magnetic resonance imaging (MRI) and temporal bone computed tomography (CT) was performed on the first day of his admission to our clinic. We initiated our standard treatment protocol for the patient (intravenous methyl prednisolone sodium succinate at 1 mg / kg for 3 days, 40 mg for 3 days, 20 mg for 3 days and 10 mg for 3 days). The patient was suspected of having cerebral venous thrombosis (CVT) due to a filling defect in the left transverse sinus in MRI. The patient was consulted to the Radiodiagnostics Department and MRI venogram was performed. CT and MRI images and findings are presented in Figure 1 and Figure 2.
As a result of these findings, the patient was diagnosed with idiopathic left‐sided SSNHL and an incidental giant arachnoid granulation. SSNHL treatment was continued. The patient was consulted to the Neurology Department for headache. The patient was diagnosed with tension headache and received medical treatment.
Informed consent form obtained from patient.
Discussion
SSNHL can be described as a sensorineural hearing loss of at least 30 dB at three consecutive frequencies within 72 hours [6]. It is well known that more than 90 percent of SSNHL is idiopathic. CVT is a cerebrovascular illness related with a wide assortment of clinical signs and indications. CVT is regularly characterized by indications such as cerebral pain, seizures, focal neurological deficits with frequent deterioration of consciousness to progressive coma and death [7]. However, CVT can also occur with nonspecific symptoms such as acute unilateral hearing loss. AGs are usually asymptomatic, and asymtomatic AGs do not requiere treatment [8]. It has been reported that arachnoid cysts may also be related to hearing loss and tinnitus [9].
AGs are unexpectedly encountered on imaging, especially on contrast enhanced CT or MRI and they must be separated from CVT. Diagnostic delay or misdiagnosis between this two entities postpones appropriate therapy. CVT is most frequently most extensive than AGs, including a complete fragment of a sinus or indeed a few sinuses. CVTs can extend into cortical veins. Acute CVT findings are noted on MRI as a high intensity CT signal and generally a high T1-weighted and low T2-weighted signal [10].
In our case, the diagnosis of SSNHL and an incidental giant arachnoid granulation was confirmed by specific MR findings. The standard treatment of CVT is anticoagulation with heparin; endovascular treatment with local intrasinus thrombolysis or mechanical thromboaspiration are the other choises [11]. Treatment options for SSNHL are systemic and topical steroids, antiviral agents, hyperbaric oxygen therapy and diuretics [6]. Therefore, it is very important to confirm the diagnosis and avoid diagnosis delay in order to provide early and correct treatment. Accurate interpretation and careful examination of MRI findings are essential for differential diagnosis of SSNHL.
Conclusion
We encountered a case of giant arachnoid granulation which can be misdiagnosed as a CVT with SSNHL. Giant arachnoid granulation should be considered as a differential diagnosis before definitive diagnosis of cerebral sinus thrombosis. MRI is the most useful diagnostic instrument to distinguish AGs from CVT.
Informed Consent
Informed consent form obtained from patient.
References
- Grossman CB, Potts DG. Arachnoid granulations: radiology and anatomy. Radiol. 1974;113:95-100.
- LeGros Clark WE. On the pacchionian bodies. J Anat. 1920;55:40-8.
- Leach JL, et al. Normal appearance of arachnoid granulations on contrast-enhanced CT and MR of the brain: differentiation from dural sinus disease. AJNR Am J Neuroradiol. 1996;17:1523-32.
- Arjona A, Delgado F, Fernandez-Remero E. Intracranial hypertension secondary to giant arachoind granulations. J Neurol Neurosurg Pschiatry. 2003;74:418.
- Trimble CR, et al. "Giant" arachnoid granulations just like CSF?: NOT!! AJNR Am J Neuroradiol. 2010;31(9):1724-8.
- Chandrasekhar SS, et al. Clinical practice guideline: Sudden hearing loss (update). Otolaryngol Head Neck Surg. 2019;161(1):1-45.
- Kuehnen J, et al. Cranial nerve syndrome in thrombosis of the transverse/sigmoid sinuses. Brain. 1998;121(2):381-8.
- Gattringer T, et al. Acute unilateral hearing loss as an early symptom of lateral cerebral sinus venous thrombosis. Arch Neurol. 2012;69(11):1508-11.
- Ottaviani F, et al. Arachnoid cyst of the cranial posterior fossa causing sensorineural hearing loss and tinnitus: a case report. Eur Arch Otorhinolaryngol. 2002;259(6):306-8.
- Deprez FC, Hernalsteen D, Bosschaert P. Arachnoid Pacchioni's granulation bulging in a transverse sinus of the brain. JBR-BTR. 2010;93(2):104.
- Mortimer AM, et al. Endovascular treatment of children with cerebral venous sinus thrombosis: a case series. Pediatr Neurol. 2013;49(5): 305-12.
|