

Authors
|
|||||||||
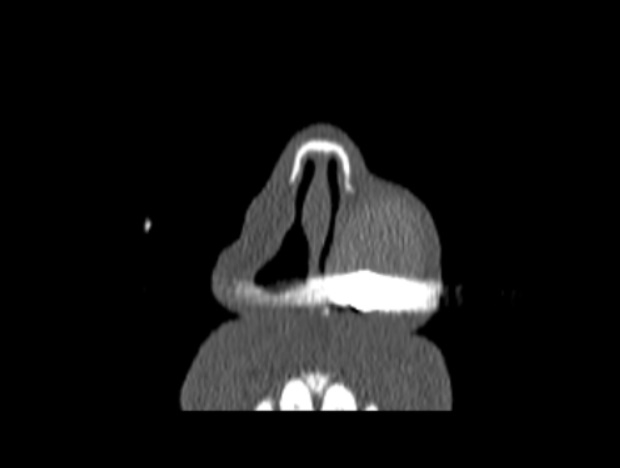
AbstractForeign bodies in the nose are relatively uncommon in adults. The presence of foul-smelling, purulent nasal discharge may be the sole symptom of a nasal foreign body. When foreign bodies are discovered incidentally, they are usually detected during the investigation of chronic symptoms. In this paper, we describe a case that is of interest due to a nasal foreign body remaining clinically silent for more than 50 years.IntroductionForeign bodies (FBs) of the nose are frequently encountered in otorhinolaryngology clinics, particularly in children. The most common age of presentation has been reported to be between 2 and 4 years [1]. FBs are commonly found anterior to the middle turbinate or along the floor of the nose, just below the inferior turbinate [2]. In rare cases, they are found in the paranasal sinuses. Patients with a nasal FB may present with several symptoms, including nasal discharge, epistaxis, infection, halitosis, foul breath, and chronic sinusitis. FBs can even cause septal perforations, synechia, and nasal stenosis [3]. Although most nasal FBs do not cause any problems and can be easily removed in the outpatient clinic, an inserted nasal FB can damage the nasal mucosa/cartilage and result in potentially serious complications [4]. Common FBs that get stuck in the nose are food, small toys, beads, insects, and worms. In this article, we describe a case of a bullet as an unusual nasal FB that had remained impacted for more than 50 years before it became clinically evident. Case ReportA 63-year-old male patient presented to our otolaryngology clinic with nasal obstruction and a foul smell emanating from his nose. These symptoms were of spontaneous onset and not associated with any other condition or precipitating event. On anterior rhinoscopy, a blackish material which was covered with exudates was seen in the left nasal vestibule anterior to the inferior nasal concha. The left nostril was fully obstructed. The right nasal cavity examination was normal. Flexible nasolaryngoscopy was performed. Other otolaryngological examinations were normal. When questioned in terms of anamnesis, the patient stated that when he was a child, he was accidentally shot in face by gunfire when walking across the street. He did not recall whether this object had ever been retrieved, and he did not seek any medical help. A computed tomography (CT) scan was ordered. The CT scan demonstrated a granulated and calcified mass measuring 2 cm x 3 cm in the left nasal vestibule (Figure 1a, Figure 1b). There was a hyperdense object measuring 8 mm x 13 mm in the center of the granulation tissue. In light of the patient’s history, this object was considered to be a bullet.
Surgical FB extraction under general anesthesia was planned. Operative findings during examination under anesthesia indicated the presence of a large occlusive FB lodged in the left nasal vestibule (Figure 2). The FB was fully extracted by nasal endoscopy. On the examination of the object, it was observed to be encrusted with a dark, friable, carbonaceous material with a solid central core, confirming that it was a bullet (Figure 3). After the successful extraction of the FB, a nasal splint was inserted to prevent synechia. The splint was removed on the seventh postoperative day. The biopsy report of the specimen showed chronic inflammatory tissue. The postoperative course was uneventful, with no nasal symptoms. All the symptoms of the patient were resolved.
DiscussionFBs in the nose are uncommon in adults. However, when located in the upper aerodigestive tract, they can be a significant cause of morbidity and mortality [5]. Unlike FBs in other parts of the aerodigestive tract, which often result in noticeable symptoms, FBs in the nose can go undetected for significant periods of time. In our patient, the FB had not caused any symptoms for more than 50 years. Several important complications may occur due to the presence of a nasal FB, including the formation and development of rhinoliths, toxic shock syndrome, and development of infections in surrounding structures, including acute sinusitis or otitis media, periorbital cellulitis, meningitis, acute epiglottitis, and tetanus [3]. The most frequent signs and symptoms after a latent period are unilateral nasal discharge, nasal obstruction, epistaxis, headache, and sinusitis. Our patient had no symptoms for 50 years, but nasal obstruction had recently become his main concern. Clinical examination, including anterior rhinoscopy and nasoendoscopy are necessary for the nasal FB diagnosis. Radiological assessment is performed if clinical examination is difficult or inconclusive. In our case, we performed anterior rhinoscopy and nasal endoscopy for the comprehensive evaluation of the bilateral nasal cavity. A blackish material covered with exudates was seen in the left nasal vestibule anterior to the inferior nasal concha. After the clinical examination, a CT scan was undertaken for further evaluation. Surgical intervention is often required for the extraction of chronic nasal FBs. In our case, we performed the endoscopic removal of the FB without any incision. The extracted FB was identified as a bullet. The use of conventional open methods for the removal of FBs can lead to increased morbidity, scaring, disfigurement, and potentially other complications [6]. Several traumatic cases of traumatic sinonasal foreign bodies have been reported. Most commonly, injuries involving high-velocity trauma, such as firearms, ballistic projectiles, and high falls, increase the risk of penetrating foreign bodies [7,8]. Firearm injuries in the craniofacial region often cause damage to vital organs, leading to irreversible and uncompensated loss and may even have fatal consequences. If the bullet does not exit the head, the most likely site of lodgment are the nose and paranasal sinuses [9]. For, FBs located in the paranasal sinuses, endoscopic transnasal surgery with the navigation system may provide a accurate localization of the FB and prevents unnecessary tissue dissection [10]. Our patient was a victim that was accidentally shot by gunfire in the face while walking across the street when he was a child. The bullet caused no symptoms for 50 years. Endoscopic removal of the FB was performed without any incision. ConclusionFBs in the nose may be undetected for significant periods of time. Clinicians should investigate the FBs in the presence of symptoms such as unilateral nasal discharge, nasal obstruction, epistaxis, headache, and sinusitis. References
|
|||||||||
| Keywords : Nazal kavite , yabancı cisim , kurşun | |||||||||




|