

|
|||||||
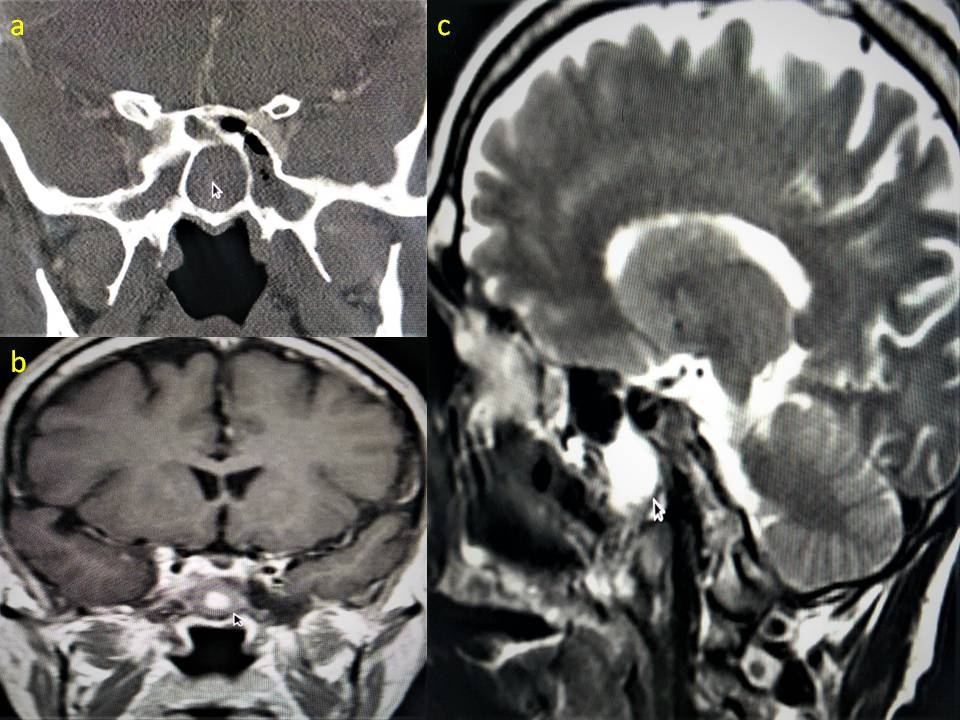
AbstractIntroduction:A sixth cranial nerve can be affected by itself in some circumstances but isolated bilateral abducens nerve palsy is rare. We report an unpublished case of bilateral abducens nerve palsy.Case: A 57-year-old male patient presented at our outpatient clinic complaining of headache and double vision. The patient then underwent endoscopic sphenoid sinus surgery. The headache that was present on the postoperative first day gradually decreased and disappeared on the second day. Discussion: Isolated bilateral abducens nerve palsy is very rare.The abducens nerve has a long course, making it more likely to be affected from such disorders. Our patient had isolated sixth nerve palsy due to a fungal etiology and underwent endoscopic surgery. Conclusion: Isolated abducens nerve palsy is rare and can be cured with emergency endoscopic surgery when due to a fungal etiology. IntroductionIsolated Abducens nerve palsy is rare in the literature and is more commonly seen in infectious diseases, trauma, tumors and intracranial diseases. The sphenoid sinus is located close to important anatomical structures such as the cavernous sinus, optic nerve, internal carotid artery, cranial nerves III, IV, V and VI. Thus, the spread of infection or inflammation to structures adjacent to the sphenoid sinus may cause serious intracranial and orbital complications. Paralysis of the cranial nerves can also be caused by benign or malignant tumors involving the head and neck. Tumors may affect the cranial nerves by local compression, direct infiltration or paraneoplastic process [1]. Any disease or condition that causes cranial nerve palsy usually affects more than one cranial nerve. The sixth cranial nerve (abducens nerve) may be affected alone in some cases, but isolated bilateral abducens nerve palsy is very rare. Isolated sphenoid sinus inflammation mostly describes pathologies such as acute bacterial sinusitis, sphenoid sinus mucocele and fungal infection [2]. Since early symptoms of sphenoid sinus diseases are usually nonspecific, this may lead to delayed diagnosis and treatment [3]. Isolated bilateral abducens nerve palsy suggests a serious intracranial event. Since the abducens nerve travels a long distance, it is likely to be affected [4]. Nontraumatic isolated abducens nerve palsy may be indirectly related to a mass stretching and compressing the nerve [5]. In this article, we present a case of isolated bilateral abducens nerve palsy due to a sphenoid fungus ball, which has not been previously published in the literature, and a case in which this pathology was completely treated with emergency surgical intervention. Case ReportA 57-year-old male patient presented to our outpatient clinic with headache and diplopia. He also had lateral gaze limitation in both eyes and was diagnosed with bilateral abducens nerve palsy of unknown etiology by an ophthalmologist. Medical history and clinical examination including detailed nasal endoscopy and other neurologic tests were nonspecific. There was no history of convulsions, head trauma, joint pain or edema. Neurologic examination revealed no evidence of cranial nerve involvement or meningitis other than bilateral lateral rectus palsy, and fundoscopic examination was normal. No etiologic cause such as trauma, vasculitis and multiple sclerosis, which are other causes of cranial nerve palsy, was found. Liver, cardiac and coagulation profiles were normal. Dengue fever, Brucella, malaria, hepatitis markers, Ebstein Barr (EBV) and Cytomegalovirus (CMV) serologies were negative. Computerized paranasal sinus tomography (CT) and magnetic resonance imaging (MRI) were performed. Both CT and MRI showed an isolated hyperintensity confined within the sphenoid sinus, noninvasive to the sphenoid sinus wall. Both sphenoid sinuses were completely affected by the disease and there was no intracranial involvement. CT and MR images are presented in Figure-1.
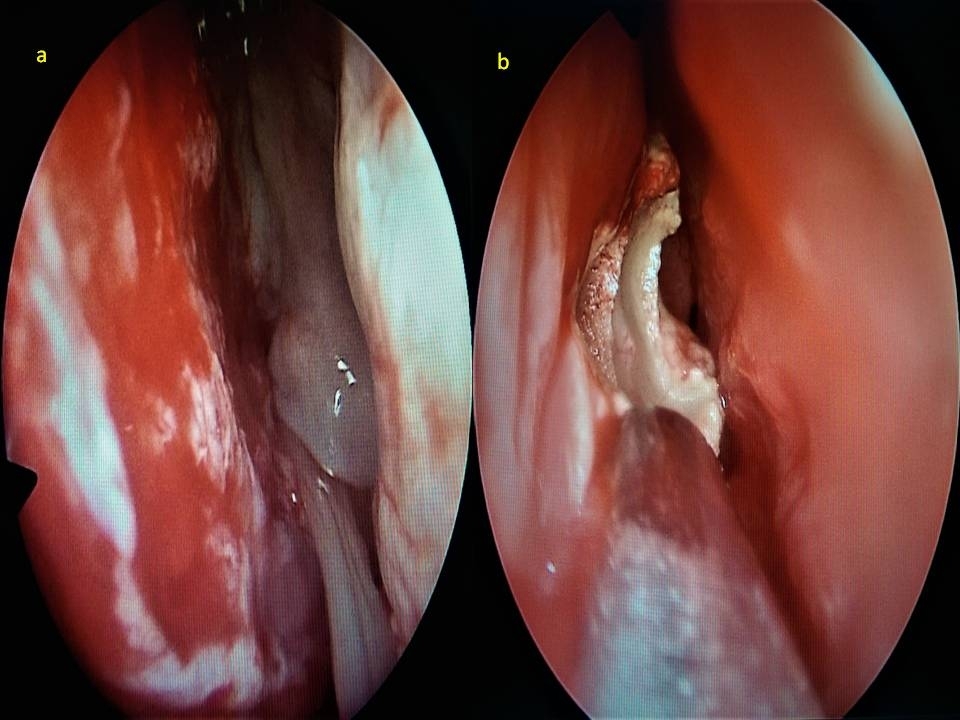
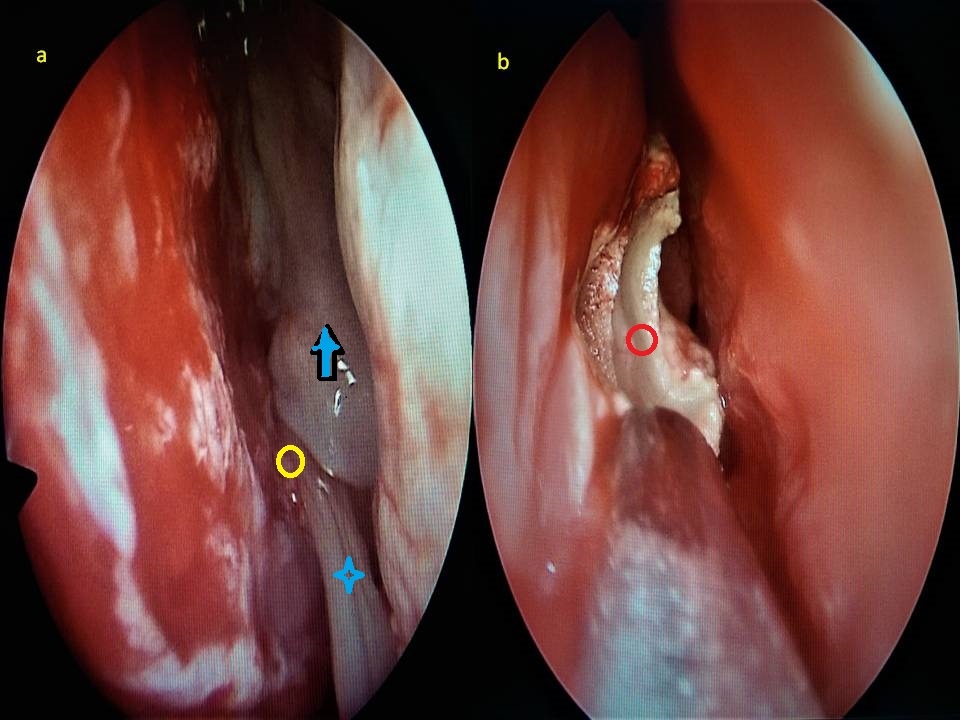
The patient was started on cefalosporin group antibiotics and steroid treatment (1mg/kg, gradually decreasing) due to neuronal paralysis, followed by endoscopic sphenoid sinus surgery. Left sphenoid ostium was dilated and the fungal material (fungal ball) in the sinus was completely excised as shown in Figure-2.
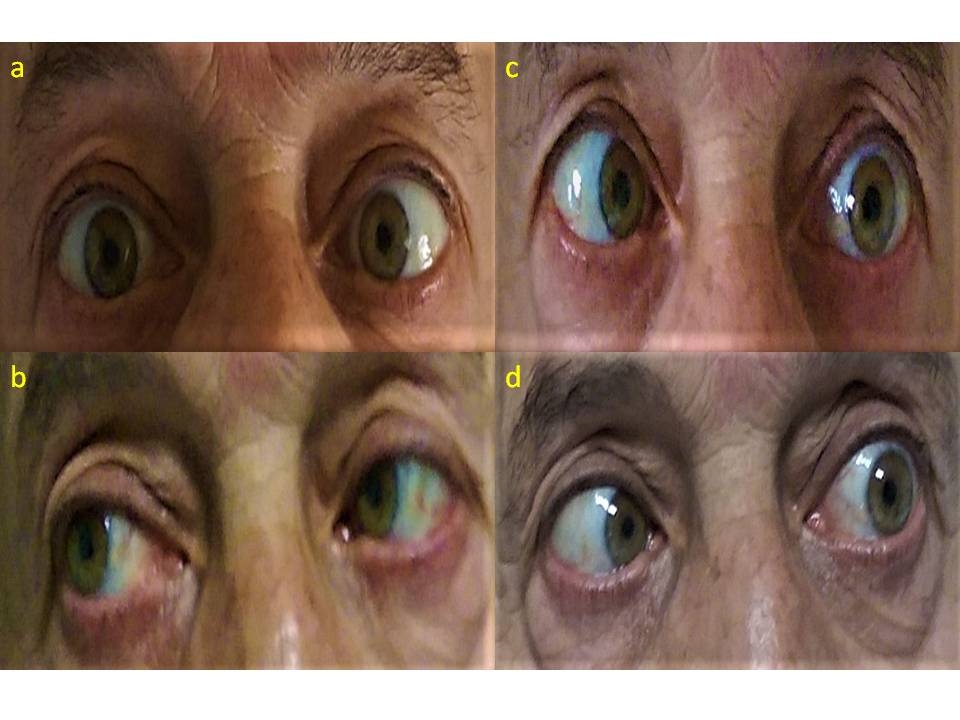
On histopathologic examination, fungal hyphae were found on PAS-Methenamine silver sections of the material. Postoperative headache which was present on the first postoperative day gradually decreased and disappeared on the second postoperative day. Double vision and abducens nerve palsy gradually improved within a week. Figure-3 shows the preoperative and postoperative images of the right and left eyes.
DiscussionIsolated bilateral abducens nerve palsy is very rare. Paranasal sinus pathologies and especially sphenoid sinus involvement may affect the abducens nerve less frequently [2]. The fact that the abducens nerve has a long course increases the possibility of being affected by such disorders [1]. However, none of these etiologies were observed in our patient. Kishimoto reported a rare orbital apex syndrome secondary to fungal septal abscess caused by S. apiospermum in a patient with uncontrolled diabetes [6]. Illing et al. also reported a case of bilateral sixth nerve palsy due to allergic fungal rhinosinusitis [2]. In our patient, fungal etiology was found and endoscopic surgery was performed and broad-spectrum antibiotic and steroid treatment was given. We found only two cases with fungal etiology in the literature. In acute fungal sinusitis, mortality rates are as high as 40% to 80% when intracranial invasion occurs [2]. Approximately 24-50% of patients may present with visual loss due to delay in diagnosis caused by nonspecific symptoms in the early stage [3]. Intracranial events such as aneurysm, subarachnoid hemorrhage, cerebrovascular accident, arteriovenous malformations, tumors, encephalitis, vasculitis and meningitis should be considered in the differential diagnosis [5]. Nandi S. et al. reported isolated bilateral abducens nerve involvement in infectious mononucleosis and demonstrated the efficacy of corticosteroid treatment [7]. The etiologies discussed above were not found in our patient. ConclusionIsolated abducens nerve palsy is rare and can be cured with emergency endoscopic surgery when due to a fungal etiology. References
Presented atIt was presented as a poster presentation at a 10th National Otology Neurotology Congress, 12th Cochlear Implantation Audiology Congress. 4-6 May 2023, Muğla, Turkey. |
|||||||
| Keywords : Bilateral Abdusens Felci , Mantar Topu , Sfenoid Cerrahisi | |||||||
|