

Authors
|
|||||||||||
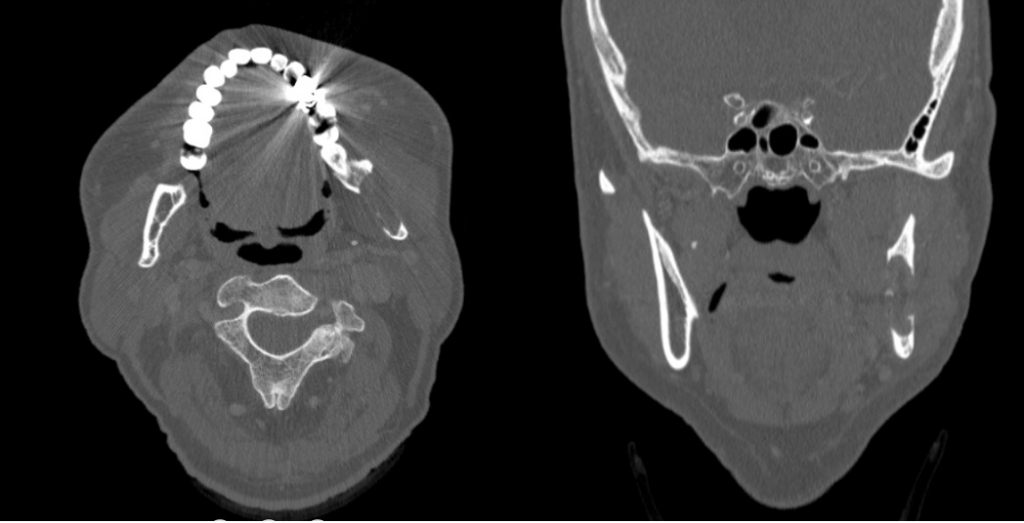
AbstractAmong the masses seen in the oral cavity, distant metastases constitute 1% of all oral cavity neoplasms. Within this 1%, renal cell carcinoma is the third most common cancer that metastasises to the oral cavity after lung cancer and breast cancer, respectively. Although thyroid, salivary glands, skull base, sinuses, pharynx, tonsils, tongue, lips and skin metastases have been reported in the literature in order of incidence, very few renal cell carcinoma mandibular metastases have been reported in the literature in the last 25 years.A patient referred to our clinic by a dentist presented with swelling on the left side of the face and a 2x3 cm radiolucent lesion in the left mandibular corpus on orthopantomogram. The patient had previously been diagnosed with renal cell carcinoma and had received chemotherapy followed by targeted therapy for one year. After advanced radiological examinations, the pathology of the biopsy taken under general anaesthesia was reported as renal cell carcinoma. By sharing this experience with clinicians, the aim is to raise awareness that metastasis of an existing malignancy should be considered in the preliminary diagnosis of patients with known malignancies other than in the head and neck region who present with swelling in areas such as the mandible where distant metastasis is uncommon. IntroductionRenal cell carcinoma (RCC) is the 13[th ]most common malignancy worldwide. Approximately 270,000 cases of kidney cancer are diagnosed every year, with 116,000 deaths due to this cancer. [1] Distant metastasis is seen in approximately 30% of RCC patients, typically in the lungs, bones, lymph nodes, adrenal glands, liver, and brain. [2] However, metastatic tumors to the oral cavity are very uncommon and represent approximately 1% of oral neoplasms. [3] Of neoplasms that metastasize to the oral cavity, renal cell carcinoma is the third most common following lung and breast carcinoma. [4] Metastasis to the head and neck region occurs in only 7.5% of RCC patients and is mainly seen in the thyroid, salivary gland, skull base, sinuses, pharynx, tonsils, tongue, lips, and skin. [5] Metastasis to the mandible is extremely rare and there have been few case reports in the literature over the last 25 years. The lesions may be asymptomatic or painful and may cause paresthesia, tooth mobility, regional lymphadenopathy, local swelling, exophytic growth, modification of the normal aspects of oral mucosa, and even pathological fractures in osseous lesions. [6] Histopathological findings are essential and generally reflect the pattern of primary tumors. [7] As these metastatic tumors are uncommon in the maxillofacial region and diagnosis can be challenging, immunohistochemical expressions can be used as an auxiliary diagnostic tool in addition to imaging examinations. [7-8] The case is here reported of a patient with RCC that metastasized to the mandible. Case ReportA 62-year-old male patient had been receiving treatment in the Medical Oncology Department for metastatic renal cell carcinoma for 6 months. In addition to lung, bone, and adrenal metastasis, a lung mass was diagnosed, and treatment of pazopanib 800 mg per day was started. During systemic treatment, grade I diarrhea occurred and this resolved without medication. After 3 months of first line pazopanib treatment, chest and abdominal computed tomography revealed partial regression and so treatment continued. In the 6th month of systemic treatment, the patient presented at the oncology clinic with the complaint of swelling in the left jawbone and was referred to the maxillofacial surgeon. Orthopantomogram examination showed a 2x3 cm radiolucent lesion on the left mandibular corpus and the patient was then referred to our hospital (Figure 1).
The physical examination showed asymmetry of the face with a bony hard swelling in the left mandibular corpus, approximately 2.5 x 3 cm in size with ill-defined borders, which was tender, immovable, non-fluctuant, non-compressible, and non-reducible in nature. The maxillofacial CT scan revealed the presence of a 20x32 mm mass located at the left mandibular angle. This mass was seen to have caused destruction of the cortex, resulting in perforation, as depicted in Figure 2.
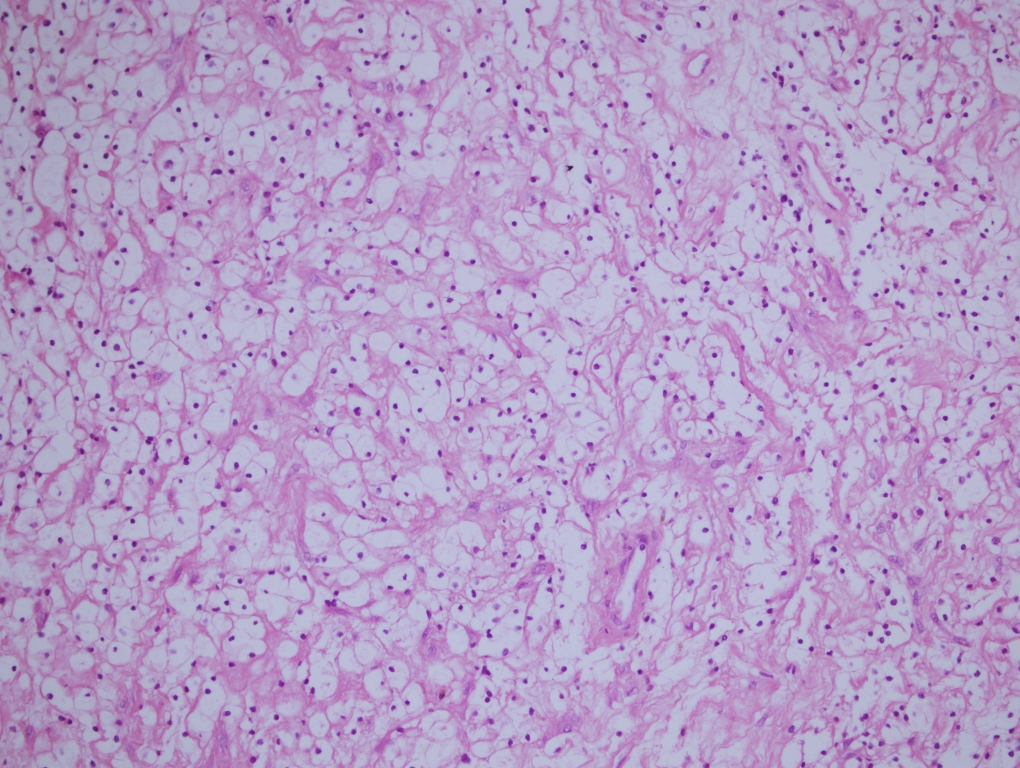
An incisional biopsy was taken under general anesthesia. Histopathological examination revealed tumor infiltration of round, polygonal cells with large clear cytoplasm and mild to moderate atypia in a thin vascular stroma (Figure 3).
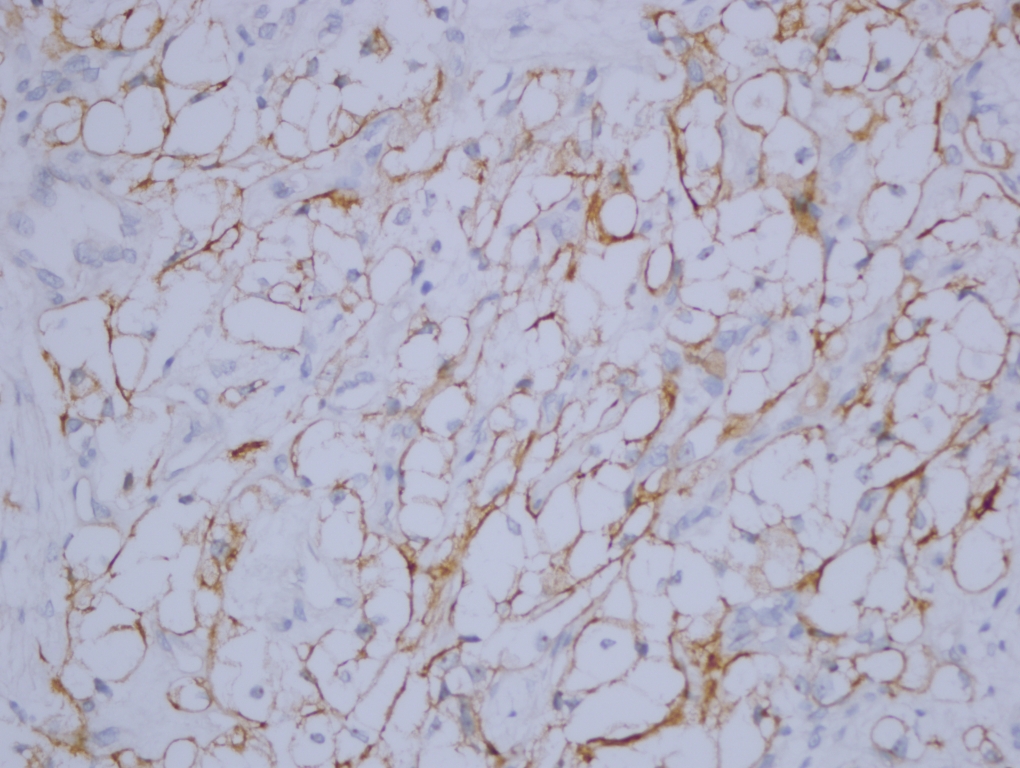
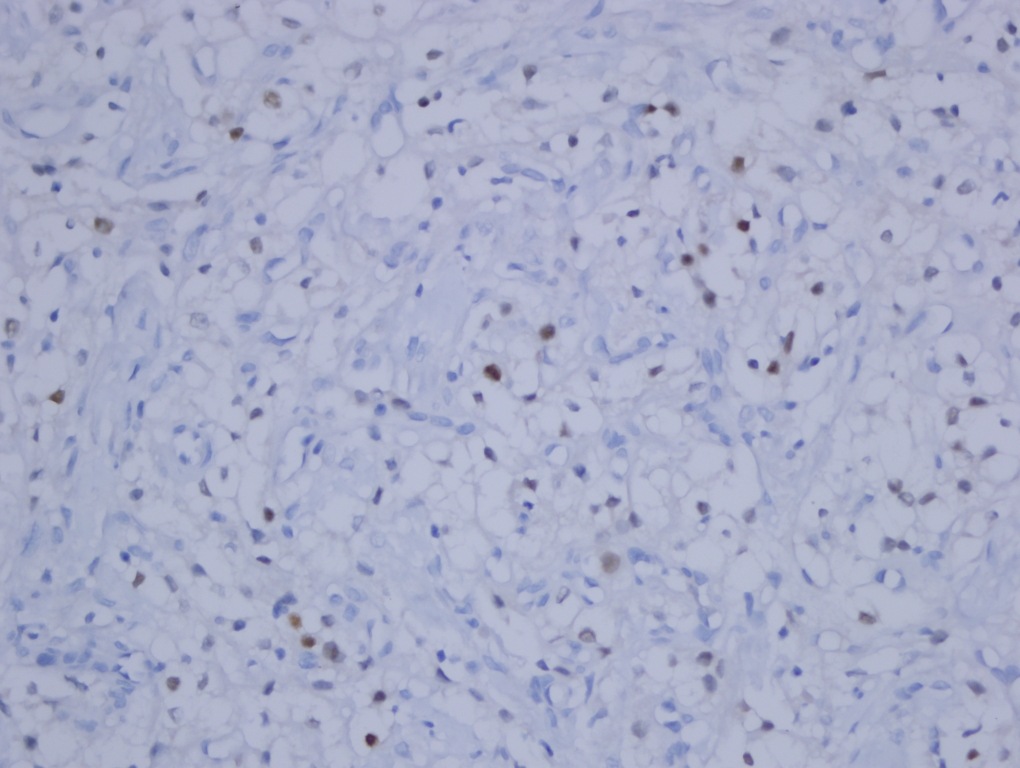
On the chest and abdominal imaging, the primary tumor and metastatic lesions were seen to be stable. The patient was discussed by the multidisciplinary Tumor Board and was considered as oligoprogressive disease. Segmental mandibulectomy or radiotherapy was offered for the metastatic lesion on the mandible, but the patient did not accept either of these options. The medical oncology treatment was then switched to nivolumab as second-line treatment. DiscussionMetastases to the oral cavity of head and neck region are extremely rare conditions [7], and metastatic tumors account for less than 1% of all oral malignancies. Rare metastasis locations include the thyroid and parotid glands, the tongue, mandible, paranasal sinuses, facial skin, and the scalp. [9] Although metastases to the orofacial soft tissues and sinuses have been well documented, involvement of the mandible is extremely rare with only a few case reports over the last 25 years. [10] Such metastases can affect males and females equally at any age. [11] Hirshberg et al. stated that the kidney is the third most common primary site for oral metastases followed by breast and lung tumors, constituting 20-30% of RCC patients diagnosed with metastasis. [12] Metastasis to the mandible is seen 4 to 5-fold more than metastasis to the maxilla. This difference is associated with the red bone marrow and the quantity of distributed blood. Renal cell carcinoma metastasizes into the head and neck region via the 3 routes of lymphatic, hematogenous, and venous route without prevertebral epidural valve (Batson plexus). [9] Clinically, orofacial metastases of renal cell carcinoma may show the following characteristics: submucosal or jaw mass, jaw or oral pain, lip numbness, gingival swelling, or a regular and extensive bilobular mass. Other signs have been reported to be bleeding, tooth mobility, trismus, paraesthesia, and paralysis. [11] CT images usually show irregular osteolytic destruction. [13] Differential diagnosis of expanding lesions of the mandible includes osteomyelitis, pyogenic granuloma, mandibular cyst, ameloblastoma, benign neoplasms, primary malignant tumors, systemic diseases with bone involvement, systemic malignancies, and metastatic malignancies. Histologically other tumors that also contain clear cells enter into the differential diagnosis, including: mucoepidermoid carcinoma, acinic cell carcinoma, odontogenic carcinoma with clear cells, and calcifying epithelial odontogenic tumor (clear cell variant). Irrespective of clinical judgement, a biopsy is needed to investigate radiolucencies of this size and nature. [14] In microscopic examination, histopathological features of RCC vary according to subtype. Among the subtypes, the most common are clear cell RCC and papillary RCC. The specimen from the current case was reported as metastatic RCC based on positive staining with markers such as vimentin and PAX-8. [15] For the treatment of metastatic RCC, surgery is considered the main treatment option.[ ]In the present case, segmental mandibulectomy was discussed in the multidisciplinary tumor council and with the patient. As thisoption was refused by the patient, it was decided to continue the current treatment of chemotherapy and molecular targeted therapy. ConclusionA case of metastatic renal clear cell carcinoma to the mandible is herein reported. Consequently, primary and metastatic tumors should be considered in the differential diagnosis of patients presenting with a mandibular mass, and the definitive diagnosis should be made from biopsy. References
Presented atThis case was presented as Poster Presentation in Baş Boyun Kanserleri Güz Okulu – Radisson Blu Hotel / Trabzon at 9th September 2023 |
|||||||||||
| Keywords : Mandibula metastazı , oral metastaz , renal hücreli karsinom , uzak metastaz | |||||||||||


|