

|
|||||||||||||
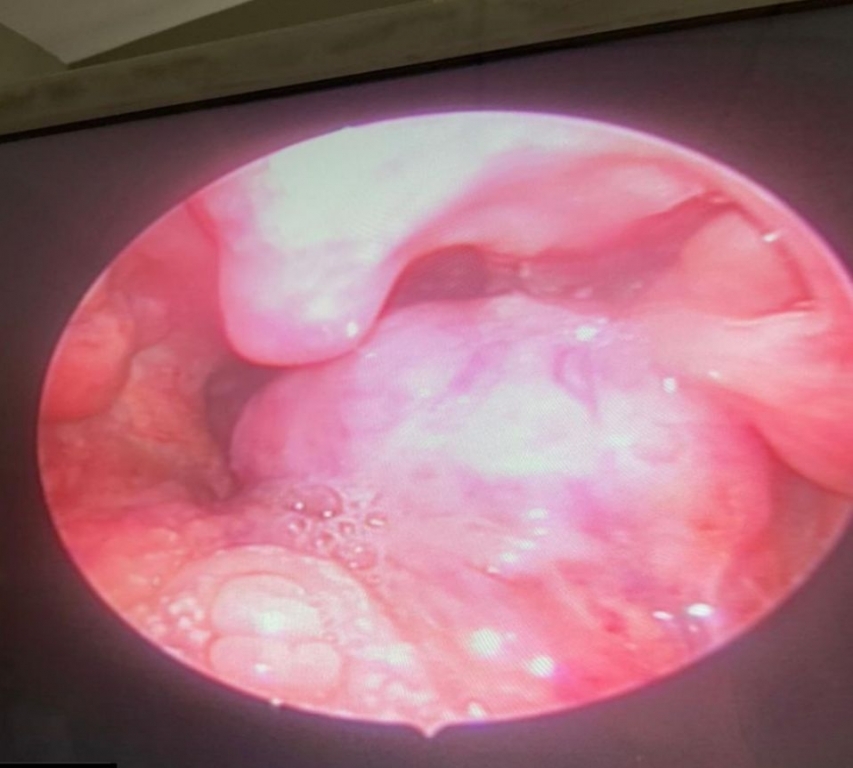
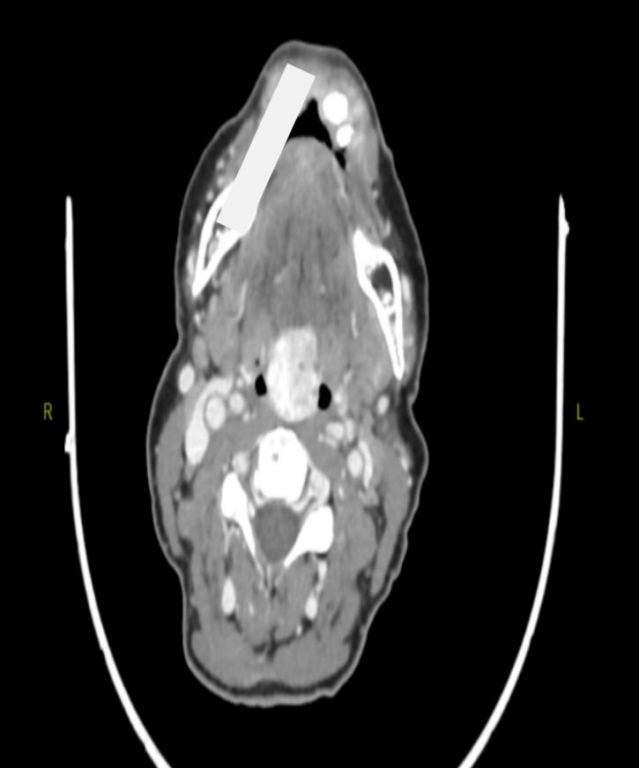
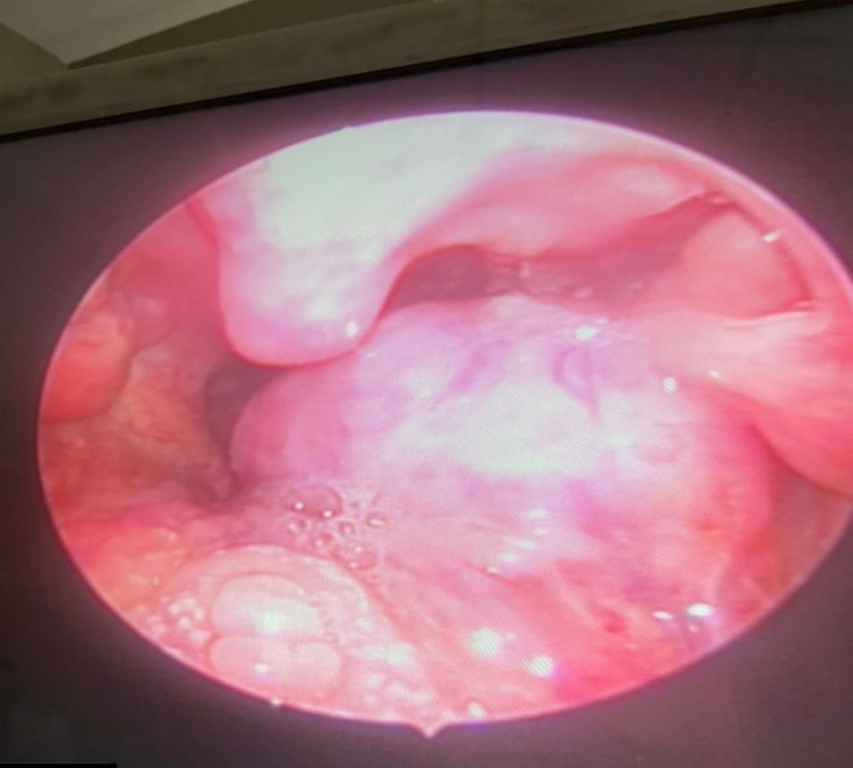
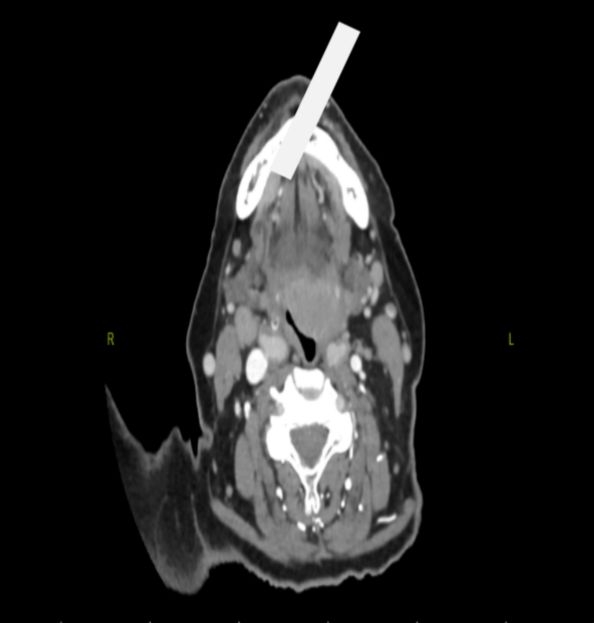
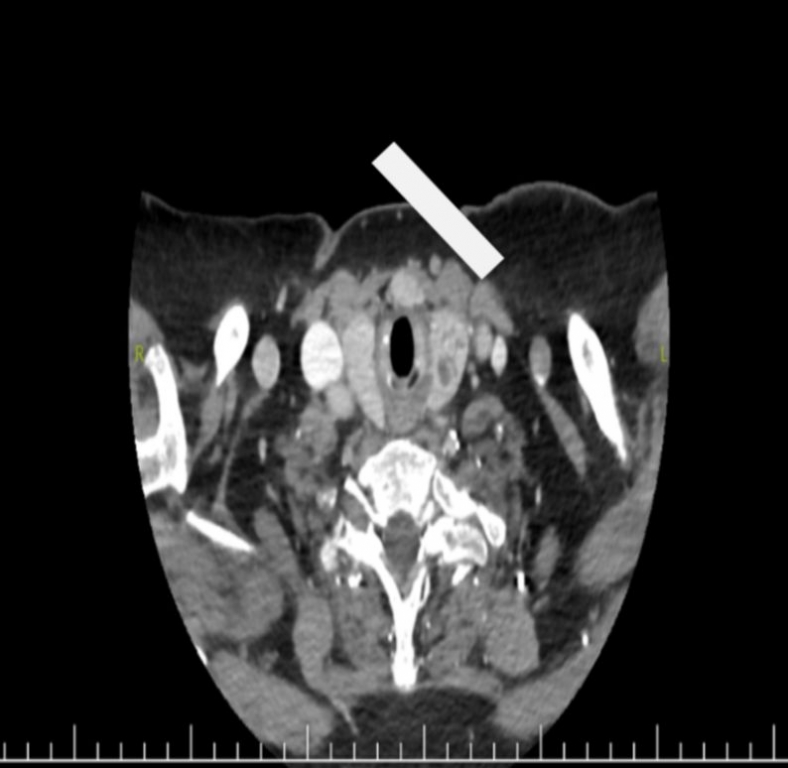
AbstractIntroduction: Ectopic thyroid is the presence of thyroid tissue outside the normal thyroid localization. The ectopically located thyroid tissue remains in the foramen caecum localization at a rate of 90% and is called the lingual thyroid.Presentation of cases: In this presentation, it is aimed to evaluate the clinical features, diagnosis and treatment processes of the mother and daughter with lingual localized thyroid tissue. Conclusion: Treatment should be planned according to the severity of symptoms, hormonal activity, and patient acceptance of treatment options. IntroductionEctopic thyroid is the presence of thyroid tissue outside the normal thyroid localization between 2-4. the tracheal rings and is one of the most common thyroid dysgenesis [1]. It mostly occurs as a result of anomalies that occur during the migration in embryological life to its normal pretracheal localization through the thyroglossal duct, starting from the foramen caecum located between the anterior 2/3 and posterior 1/3 of the tongue [2]. Its prevalence has been reported as 1/100.000-300,000 [1]. The ectopically located thyroid tissue remains in the foramen caecum localization at a rate of 90% and is called the lingual thyroid [3]. Other locations are on the migration line of the thyroid tissue, but there are also distant locations. Heart, aorta, esophagus, duodenum, gallbladder, stomach, pancreas, adrenal gland, ovary, fallopian tubes and thyroid tissue located in the vagina have also been reported [1]. Ectopically located thyroid, although usually asymptomatic, can also cause clinical symptoms of hypothyroidism such as dysphagia, dysphonia, upper airway obstruction, cold intolerance, weakness, weight gain, fatigue, and constipation [4]. In this presentation, it is aimed to evaluate the clinical features, diagnosis and treatment processes of the mother and daughter with lingual localized thyroid tissue. Case ReportCase-1 A 41-year-old female patient (daughter) was admitted to our clinic with complaints of swelling behind the tongue, choking while eating, and difficulty in swallowing. She did not have any systemic diseases and her family history was unremarkable. In the physical examination, there was a 2*2 cm lesion located on the right side of base of the tongue, covered with vascularized mucosa, filling the oropharynx approximately 25% (Figure 1A). Other ENT examinations were normal. In the neck examination, the thyroid gland was not palpable in its natural localization. In the neck ultrasonography, the left lobe was 17x6 mm in size and a 12x6 mm anechoic cystic nodule with lobulated contours was observed in it. The thyroid function tests were TSH: 11.23 mIU/L, T3: 3.32 mIU/L, T4: 0.95 mIU/L. Contrast-enhanced neck computed tomography revealed a 26 mm, hyperdense, hypervascular, and oval-shaped lesion at the base of the tongue (Figure 1B). No parenchyma was observed on the right side (Figure 1C). In the thyroid scintigraphy performed with Tc 99m, no activity involvement was observed in the thyroid gland site in the neck. In addition, focal activity involvement, which may belong to ectopic thyroid tissue (lingual thyroid?), was noted in the area that corresponds to the base of the tongue in the midline superior part of the neck. The patient, who partially closed the oropharynx but did not cause severe respiratory distress, was followed up with the Endocrinology clinic.
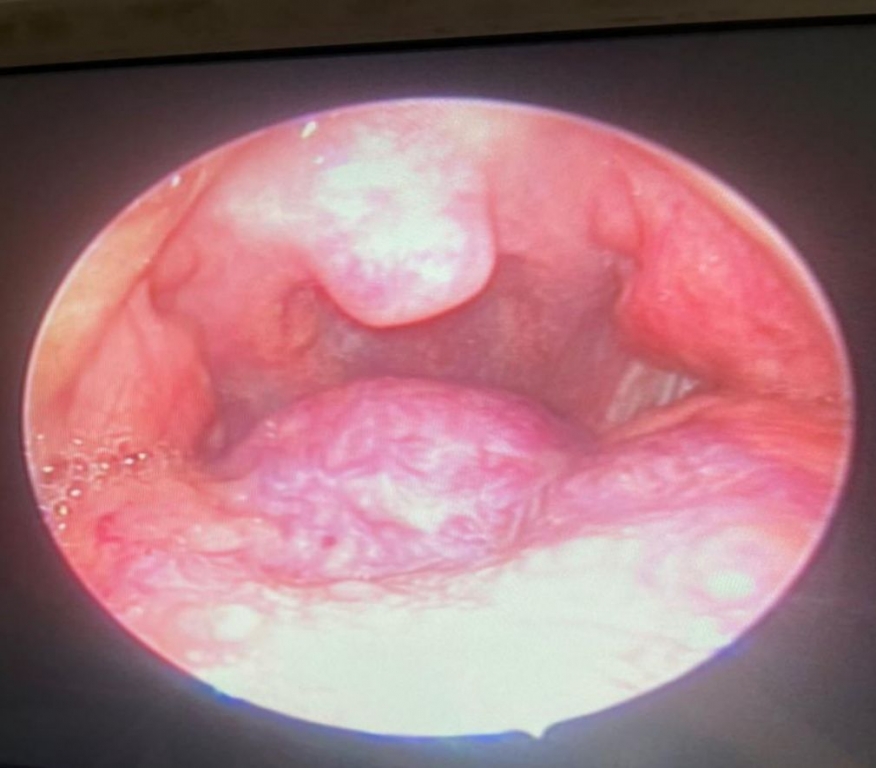
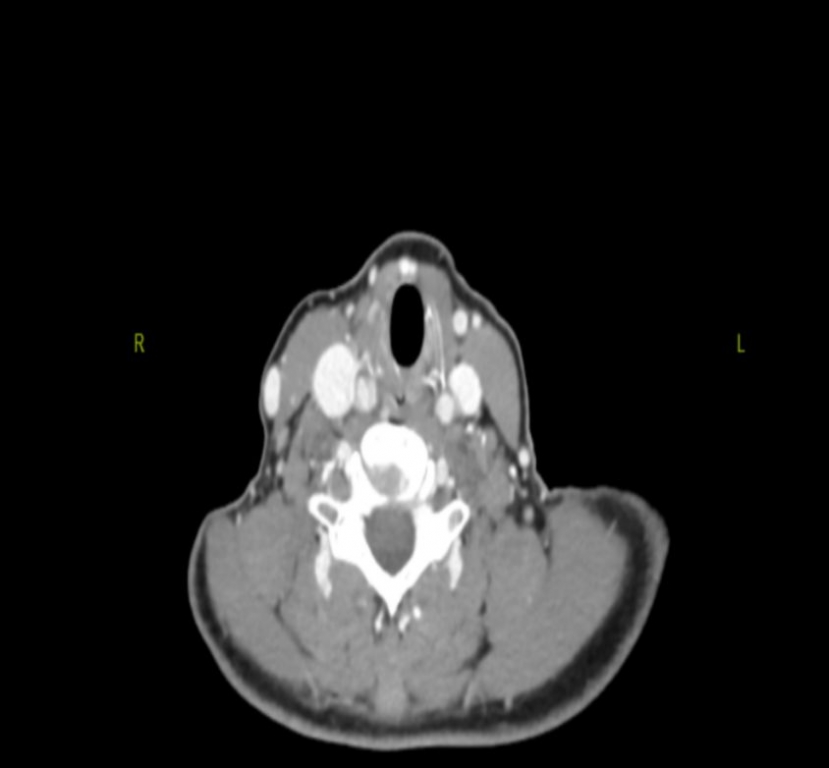
Case-2 An 87-year-old female patient (mother) admitted to our clinic with complaints of dysphagia and dyspnea. In the physical examination, there was a lesion of 3*3 cm in size, vascularized, filling approximately 75% of the oropharynx at the base of the tongue on the left (Figure 2A). Other ENT examinations were normal. The thyroid was palpated in its localization. In neck ultrasonography, the dimensions of the right lobe of the thyroid gland were 42x18x19 mm, and the dimensions of the left lobe were 49x20x22 mm. The isthmus thickness was measured as 5.5 mm. A well-circumscribed, heterogeneous hyperechoic nodule of 20x15 mm with thin hypoechoic halo was observed in the left lobe midzone. In addition, several well-circumscribed isoechoic nodules were observed in the right lobe, the largest of which was 8 mm in diameter in the isthmus. The thyroid function test was TSH: 1.67 mIU/L. On contrast-enhanced neck computed tomography, a hypodense lesion of 3 cm in size was observed in the posterior of base of the tongue on the left. At this level, the air column was narrowed (Figure 2B). Hypodense nodules were observed in the left thyroid lobe (Figure 2C). In the thyroid scintigraphy performed with Tc99m, increased activity involvement, which may be related to a hyperactive nodule in the middle part of the right lobe of the thyroid gland, was noted. The distribution of activity in other parts of the gland is homogeneous and the uptake was within normal limits when compared to submandibular glands. No activity involvement was observed in the ectopically located thyroid tissue. Surgical operation was planned due to the presence of lingual thyroid filling the oropharynx and causing respiratory distress in the patient with a normal location, functional thyroid tissue and thyroid function tests within normal limits.
Treatment and Prognosis In Case 1, preliminary follow-up was considered because of hypogenesis and non-functionality of the thyroid tissue in its normal anatomical localization, and active thyroid tissue located at the base of the tongue did not cause significant symptoms in the patient. The patient was referred to the Endocrinology department in terms of thyroid hormone regulation. In case 2, the thyroid tissue was in normal anatomical localization, normal dimensions and functional. Ectopic thyroid tissue located at the base of the tongue was not active in the scintigraphy. Surgery was recommended to the patient for ectopic thyroid tissue, which was dysfunctional and caused respiratory distress, but the patient did not accept surgery. DiscussionEctopic thyroid is a rare thyroid dysgenesis that occurs due to anomalies in thyroid gland migration during embryogenesis and is frequently seen in lingual localization. Although its pathogenesis is not known exactly, it is thought to occur due to an error in TTF-1 and TTF-2 transcription factors [5]. Its prevalence varies between 1/100,000-300,000[1]. It is seen 4-6 times more frequently in women and is often diagnosed in the second decade [6]. Although it is often asymptomatic, it may cause complaints such as dysphonia, airway obstruction, shortness of breath and dysphagia due to mass effect [4]. Patients may present with symptoms of hypothyroidism in cases where there is no thyroid tissue in its normal localization or it is non-functional and ectopic thyroid is nonfunctional [7]. Ectopic thyroid tissue can be functional or nonfunctional. Benign and malignant lesions, vascular tumors, teratomas, telangiectatic granuloma should also be considered in the differential diagnosis of ectopic thyroid gland located at the base of the tongue [8]. In addition, neoplastic formations seen in normal thyroid tissue and other diseases of the thyroid gland can be seen in ectopic thyroid [9]. Physical examination and imaging methods such as ultrasonography, CT, MR and thyroid scintigraphy can be used for diagnosis. Imaging methods are also important in determining the boundaries of the lesion. In the presence of clinical suspicion, fine-needle aspiration biopsy can also be performed for diagnosis [10]. Lingually located thyroid tissue was detected in a mother and her daughter who applied to our clinic with similar complaints. This shows that there may be genetic factors in the pathogenesis. In the first case, although scintigraphic activity was detected in the lingual thyroid tissue, subclinical hypothyroidism was detected in thyroid function tests, and was referred for medical treatment. In the second case, the thyroid was in its normal location and size and the function was normal. Ectopic thyroid can be followed if asymptomatic. If symptomatic, thyroid hormone suppression therapy can be used to reduce the mass effect and collapse the lesion [2,10]. Radioiodine treatment or surgical treatment can be considered in cases of respiratory distress, difficulty in swallowing, and in cases where reduction cannot be achieved with suppression therapy. In cases such as suspected malignancy, bleeding, ulceration, surgical treatment can be applied with a transoral or external approach [1,11]. ConclusionAlthough ectopic thyroid is a rare condition, it is one of the most common thyroid dysgenesis. Ectopic thyroid tissue may show symptoms according to location and size. Treatment should be planned according to the severity of symptoms, hormonal activity, and patient acceptance of treatment options. Informed ConsentTwo patients were mentioned in the case report and consent was obtained from both of them.References
|
|||||||||||||
| Keywords : ektopik tiroid , hipotiroidizm , lingual tiroid , tiroid disgenezisi , tiroid bezi. | |||||||||||||
|