

Authors
|
|||||||||
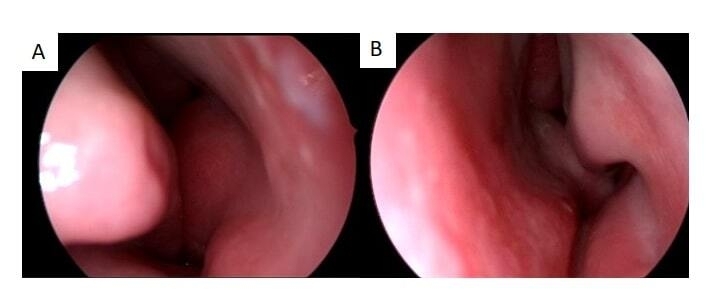
AbstractCemento-ossifying fibroma is a fibro-osseous lesion that typically occurs in the jaw bones as well as in atypical areas. If not treated, these lesions can expand to large sizes and cause deformities in the surrounding tissues. In this case, though never reported as a site of involvement before, cemento-ossifying fibroma of the nasal septum was diagnosed in a 7-year-old male patient. Examination, radiographic, histological findings and surgical treatment of the patient who applied with the complaint of nasal congestion are presented.IntroductionCemento-ossifying fibroma [COF] is a rare and benign jaw tumour stemming from the periodontal ligament, and resulting in the replacement of normal bone by fibrous tissue and calcified material [1, 2]. It has a quite sporadic percentage among odontogenic tumours. It more frequently occurs between the second and fourth decades of life and there is a female gender predominance. It is most commonly found in the posterior part of the mandible [3]. The size of ossifying fibromas can vary between 0.02 and 15 cm [4]. The differential diagnosis comprises other lesions including radiopacities within a round radiolucent mass: osteosarcoma or chondrosarcoma, odontogenic cysts, fibrous dysplasia, calcifying odontogenic cysts, calcifying epithelial odontogenic tumours and squamous cell carcinomas. The factor that can differentiate cemento-ossifying fibroma from aggressive sarcomas and carcinomas is its well-defined border. Fibrous dysplasia features a “ground glass” appearance that is not found in cemento-ossifying fibroma [5]. Only one case of cemento-ossifying fibroma transform into low-grade osteosarcoma has been reported in the literature [6]. We aimed to present the nasal septum location of cemento-ossifying fibroma, which has never been reported before in any patient in the adult or paediatric age group, to the literature. Case ReportA 7-year-old male patient was referred to us with the complaint of increasing difficulty in breathing through the nose for the last 1 month. The patient had no further complaints in his history other than nasal congestion. There were no pathological characteristics in the patient's medical and family history. In the course of the endoscopic examination, a well-circumscribed submucosal swelling was noticed in the posterior part of the nasal septum, narrowing the bilateral nasal passages(Figure 1). The subsequent head and neck examination was typical.
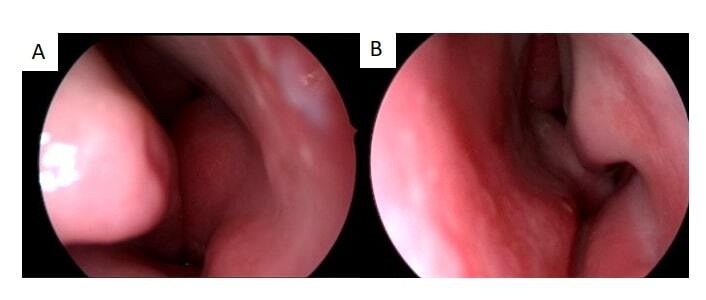
In the contrast-enhanced facial Magnetic Resonance (MRI) imaging taken at an external centre; A mass with a size of 19x26 mm was observed in the midline of the nasal septum, slightly hypointense in T1 and T2 series, smooth-contoured, and displayed minimal enhancement after intravenous (IV) contrast(Figure 2).
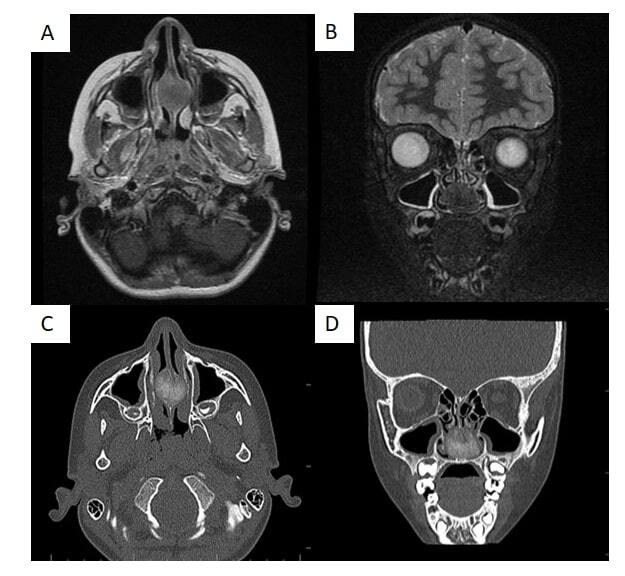
In the treatment, total endoscopic excision of the mass was planned. A submucosal entry was made in the area where the mass was located, and after the bilateral nasal septum mucosa was elevated, the fragile cartilaginous mass in the bone septum and the thin bone tissues surrounding these tissues were completely excised(Figure 3). The remaining maxillary base mass was removed with the help of a drill. The mucosa was then replaced and the operation was completed after buffering.
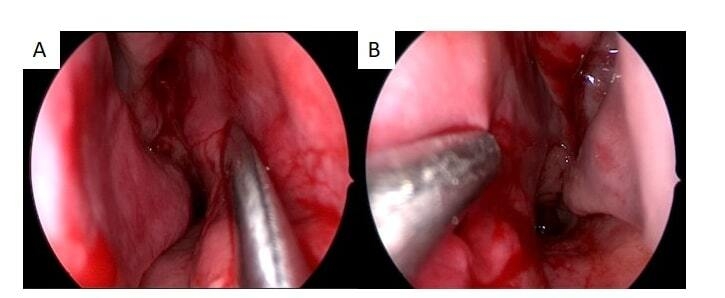
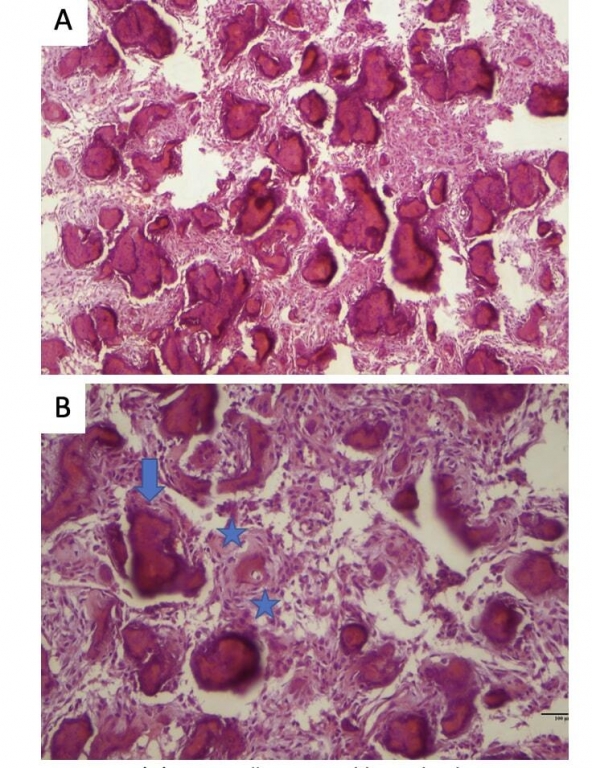
In the pathological examination of the material taken, while benign spindle stromal cells and bone structures were observed at x10 magnification, cementum-like structures and areas compatible with cemento-ossifying fibroma rich in benign spindle cells were observed at x20 magnification(Figure 4). When the pathological data were examined, it was seen that the excised material was compatible with cemento-ossifying fibroma.
Verbal informed consent was taken from the patient. DiscussionCemento-ossifying fibroma is categorized as a mesenchymal origin benign odontogenic tumour in the 4th edition (2017) of the World Health Organization [WHO] Classification of Head and Neck Tumours. The frequency of COF among all odontogenic tumours is known to be 3.5% [7]. It is widespread in the 2nd - 4th decades of life and in women. COF cases observed in the elderly and paediatric age groups are rare [3,8]. Contrary to the literature data, our patient was 7 years old and COF cases were very rare in this age group. Tumour location is primarily observed in the posterior mandible and less frequently in the maxilla. They cause expansion of the cortical bone without creating a defect in its cortex. They tend to grow slowly, and are often asymptomatic until they end up with visible deformities such as facial asymmetry and tooth displacement [8]. In our case, the tumour was located in the nasal septum, which, as far as we know, has not been reported before in the literature, and the nasal congestion was the reason for applying to the outpatient clinic. It was seen in the tumour’s Computed Tomography (CT) examination that it was an expanding lesion with mixed radiodense and radiolucent areas and a well-defined border. There was an intermediate signal in T1-weighted MRI, and a higher signal was observed in T2-weighted MRI in the non-ossified areas of the tumour as well as a lower signal in the ossified regions [9]. Coronal and axial sections of CT and MR images of our case are shown. The pathological examination of cemento-ossifying fibroma includes irregularly shaped calcifications within a hypercellular fibrous connective tissue stroma. The appearance of calcifications is extremely inconsistent and shows different stages of bone and cementum deposition. The discrimination of cementum and osteoid is histologically challenging [5]. In the diagnosis of ossifying fibroma, the characteristic microscopic appearance of fibrous tissue of inconsistent cellularity, in which some areas are almost acellular and others are densely packed with cells and a mineralized component, is taken as a basis [8,9]. In the pathological examination of the case we presented, findings rich in stromal cells, fibroosseous lesion, cementum-like bone structures and benign spindle cells were detected in consistent with the literature. The aim of treatment is to conduct complete excision in order to inhibit further expansion when possible. When tumours are small and well circumscribed, enucleation and curettage are the preferred treatments. Following the resection, the recurrence rates vary between 30% and 56% [10]. In our case, the mass was completely excised alongside the surrounding bone tissue, and the maxillary base was circumscribed to inhibit recurrence. ConclusionThis is the first cemento-ossifying fibroma case seen in the nasal septum and reported in the literature when both paediatric and adult age groups are included. Informed ConsentVerbal informed consent was taken from the patient.References
|
|||||||||
| Keywords : sementoosfiye fibrom , nazal septum , odontojenik tümör , fibroosseöz lezyon | |||||||||
|