

Authors
|
|||||
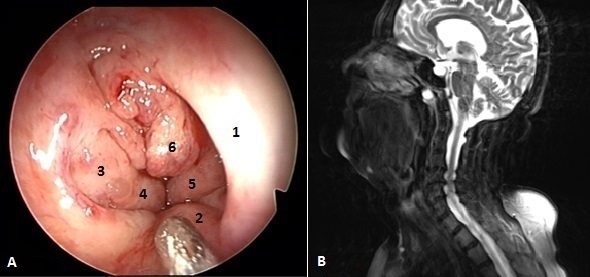
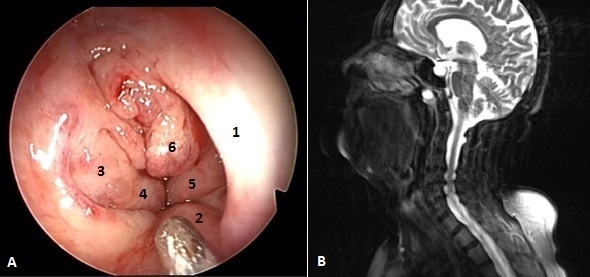
AbstractPurpose: To present a case of concomitant parotid basal cell adenoma and nasopharyngeal Warthin tumor.Characteristics of the Case: A 70-year-old female presented with complaints of snoring and swelling in the cheek. Physical examination showed a firm, fixed mass of approximately 1.5cm in size in the left parotid region. Nasopharyngeal endoscopy revealed a puffy mass that is in the midline and the same color as the surrounding mucosa on the posterior wall of the nasopharynx. While biopsy of the nasopharyngeal mass was compatible with Warthin tumor, fine needle aspiration biopsy(FNAB) of the mass in the parotid gland was compatible with pleomorphic adenoma. Treatment and Prognosis: Left superficial parotidectomy and endoscopic transnasal excision of the mass in the nasopharynx was performed. The pathology result of the nasopharyngeal mass was reported as "Warthin tumor", while the pathology result of the parotid mass was reported as "basal cell adenoma". Approximately two years after operation, there was no sign of recurrence and follow-up is continued. Comment: While examining patients with head and neck tumors, we must remember that concomitant tumors may exist in the same patient and benign salivary gland tumors should be included in the differential diagnosis of masses located in the nasopharynx. IntroductionWarthin tumor is a benign salivary gland tumor, and it’s the second most common benign tumor of the parotid gland after pleomorphic adenoma. Some cases have been reported in unusual regions such as cervical lymph nodes, submandibular glands, lips, buccal mucosa, tongue, and hard palate. Warthin tumor in the nasopharynx is extremely rare [1]. Basal cell adenoma is a rare benign salivary gland tumor. It is most commonly located in the parotid gland. In this case report, we present a patient with basal cell adenoma in the parotid gland and an accompanying Warthin tumor in the nasopharynx. Case ReportA 70-year-old female came to our outpatient clinic with snoring and left cheek swelling. She had these complaints for the last year. Her comorbidities were hypertension, chronic obstructive pulmonary disease, and diabetes mellitus. She had a history of smoking 50 packs / year. A hard, fixed mass approximately 1.5 cm in diameter was palpated in the left parotid gland. Magnetic resonance imaging (MRI) showed a 9x10x12 mm-sized mass located in the anterior part of the left superficial parotid gland. Endoscopic examination revealed a mass on the midline of the nasopharynx. The mass was the same color as the surrounding mucosa, puffy from the surface [Figure 1a]. MRI showed a 9-mm-sized, hyperintense lesion on the posterior wall of the nasopharynx at T2-weighted images [Figure 1b]. The pathology result of the fine needle aspiration biopsy (FNAB) of the left parotid mass was reported as a "pleomorphic adenoma". The result of the nasopharyngeal punch biopsy was a "Warthin tumor". We planned left superficial parotidectomy and endoscopic transnasal excision of the nasopharyngeal mass in the same session.
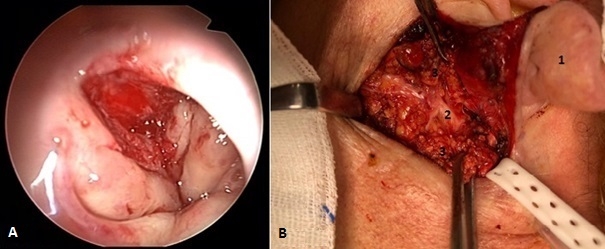
Under general anesthesia, the mass in the nasopharynx was viewed with a zero-degree endoscope and excised with punch forceps. The remaining residual tissues were cleaned using a shaver until the healthy mucosa was seen [Figure 2a]. We then initiated the superficial parotidectomy procedure. After the modified Blair incision, the facial nerve and its branches were exposed. The mass measured 2x1x1 cm located in the anterior part of the parotid gland was included in the superficial parotidectomy specimen and removed together [Figure 2b].
The pathology results showed that the patient’s nasopharyngeal mass biopsy was consistent with a Warthin tumor, and left superficial parotidectomy material was reported as basal cell adenoma. The patient continues her follow-up in the 24[th] month since surgery. There was no sign of recurrence in the nasopharynx or left parotid gland during this period. DiscussionWarthin tumor (adenolymphoma, papillary cystadenoma lymphomatosum, cystadenolymphoma) is one of the most common benign salivary gland tumors. It’s usually located in the parotid gland [1]. Although benign salivary gland tumors are more common in women, Warthin tumors are more common in men aged 55-70. It has been proven that it is directly linked to smoking [2, 3]. Our case was a 70-year-old female patient with a smoking history of 50 packs/year. The pathogenesis of the nasopharyngeal Warthin tumor is still unclear. Extraparotid Warthin tumors may develop from minor salivary gland components in the pre-existing lymphoid stroma. The nasopharynx has a lot of lymphoid tissues and some minor salivary glands. According to a study, chronic inflammation in the nasopharynx may be inducing oncocytic metaplasia in the glandular tissue in the stroma [1, 5, 8]. Nasopharyngeal tumors are mostly malignant. Benign masses are angiofibroma, chordoma, craniopharyngioma, and pleomorphic adenoma. Warthin tumor of the nasopharynx has been reported rarely in the literature [4]. Basal cell adenoma consists of monomorphic groups of basaloid epithelial cells and constitutes approximately 1-2% of all salivary gland tumors. The most common location is the parotid gland. It usually presents as a hard, mobile, and slow-growing mass [9]. The primary treatment method is surgical excision. Its prognosis is generally good, and its recurrence rate is high [13]. In our case, the basal cell adenoma located in the parotid gland showed a slow-growing course. Treatment was performed by superficial parotidectomy, and no recurrence was observed in a 24-month follow-up. There are a few cases in the literature regarding the location of the nasopharyngeal Warthin tumor. It is usually located on the right or left side of the posterior wall of the nasopharynx (Rosenmüller fossa region) [1, 4, 5, 15] and, in some cases, in the midline [16]. In our case, the nasopharyngeal Warthin tumor was in the midline and did not obstruct the eustachian tube orifice. Various cases have been reported in the literature about concomitant tumors found in both the nasopharynx and parotid gland [1, 5, 14, 15]. In these case reports, Warthin tumors in both the nasopharynx and parotid gland are presented. In our case, a nasopharyngeal Warthin tumor and an accompanying parotid basal cell adenoma were detected, both of which are very rare. In the literature, there has been no previous publication involving two different salivary gland tumors in both the nasopharynx and the parotid gland at the same time. ConclusionClinicians should consider the possibility of benign salivary gland tumors, like Warthin's tumor, in patients presenting with a nasopharyngeal mass. In addition, in patients presenting with head and neck tumors, it is important to perform a complete ear, nose, and throat physical examination, including endoscopic examinations, considering that there may be other tumors accompanying the existing tumor. AcknowledgementConflict of interest: The authors declare no conflict of interest.
Ethical Approval: All procedures were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration. This article does not contain any studies with animals performed by any of the authors.
Informed Consent: Informed consent was obtained from the participant. Informed ConsentFrom patientReferences
|
|||||
| Keywords : parotis , nazofarinks , warthin , bazal hücreli adenom | |||||
|