

|
|||||
AbstractPyogenic granuloma is a benign, proliferative fibrovascular lesion that primarily affects the skin and mucosa. Histologically, it is characterized by marked vascular proliferation. While it is most commonly found in the oral cavity, its occurrence in the nasal cavity is relatively rare. During pregnancy, it is specifically termed pyogenic granuloma gravidarum(PGG). A variety of treatment modalities are available, including surgical excision, diode laser therapy, cauterization, embolization, silver nitrate cauterization, cryotherapy, and topical therapies. This article presents a case of a giant PGG that exhibited progressive growth into the third trimester, resulting in recurrent epistaxis, significant cosmetic concerns, and nasal obstruction. Notably, the lesion did not regress postpartum, necessitating further clinical intervention.IntroductionInitially described by Poncet and Dor in 1897, the condition was first termed botryomycosis hominis due to its presumed fungal etiology. Although later studies confirmed that the lesion is neither granulomatous nor pyogenic, the term "pyogenic granuloma"(PG) has remained in use. Histopathologically, PG is classified as a lobular capillary hemangioma[1,2]. PG represents a benign fibrovascular proliferative lesion originating from the skin and mucous membranes, predominantly in the head and neck region. While it is most commonly observed in the oral mucosa, its occurrence in the nasal cavity is relatively rare. Although the exact etiology remains unclear, PG is commonly associated with trauma, hormonal fluctuations, and immunosuppression[3-4]. PG is more prevalent among women, particularly during pregnancy, when it is referred to as pyogenic granuloma gravidarum(PGG). When located in the nasal cavity, it typically presents with epistaxis and nasal obstruction. The lesion most frequently arises in the third trimester and often resolves spontaneously postpartum. However, in symptomatic cases, surgical excision remains the preferred treatment option. The decision to proceed with surgical intervention is influenced by gestational age, anticipated blood loss, and the patient's clinical status[2,5]. This article presents a case of a giant PGG that exhibited progressive growth throughout pregnancy, leading to a range of symptoms, including significant cosmetic concerns, nasal obstruction, and recurrent epistaxis. Notably, these symptoms persisted beyond the postpartum period, necessitating further clinical management. Case ReportA 29-year-old female patient presented in the third trimester of pregnancy with a rapidly growing mass originating from the left nasal cavity. The mass protruded externally and was associated with frequent episodes of bleeding. It had previously been excised at an external center but demonstrated rapid recurrence. Notably, the patient experienced significant hemorrhage from the mass during childbirth. On anterior rhinoscopy, the lesion’s size and its complete occlusion of the nasal vestibule obscured the precise site of origin. The mass exhibited areas of active bleeding and blood crusting on its surface. Endoscopic examination revealed that it occupied the anterior third of the nasal passage, causing expansion of the nasal vestibule and protruding approximately 4–5 cm beyond the passage. The posterior two-thirds of the nasal passage and the nasopharynx appeared uninvolved. Based on these findings, the mass was suspected to originate from the anterior third of the septum (Figure 1).
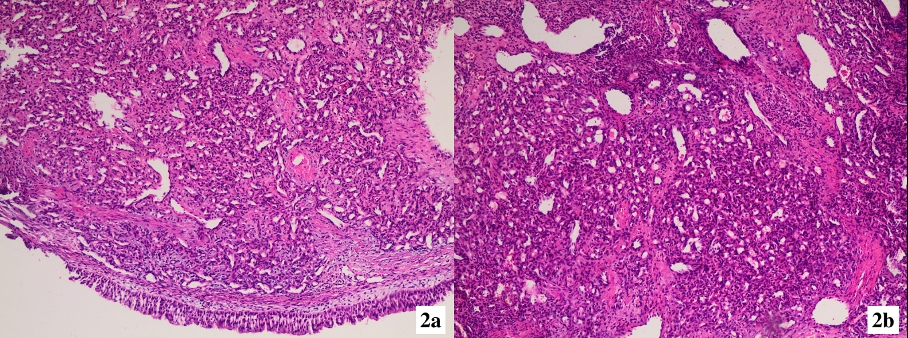
Surgical excision was performed under sedation and analgesia in an operating room setting. The mass was removed along with the involved septal mucosa, mucoperichondrium, and cartilage, ensuring a 4 mm margin of normal mucosa in the subperichondrial plane. Histopathological examination confirmed the diagnosis of lobular capillary hemangioma(Figure 2).
At the one-year postoperative follow-up, no residual or recurrent mass was detected. The patient remains under ongoing surveillance. DiscussionThe etiology of PG remains unclear; however, it has been associated with several factors, including local trauma, maceration, immunosuppression, and hormonal influences. PG predominantly affects women and typically presents in the third or fourth decade of life [2]. It primarily occurs in the head and neck region, particularly in the oral cavity, while its occurrence in the nasal cavity is relatively rare. Patients commonly present with symptoms such as epistaxis, nasal obstruction, and nasal discharge[6]. Clinically, PG typically appears as a pedunculated, hypervascular polypoid mass with an irregular surface, exhibiting colors ranging from gray-pink to red or dark, often covered with fibrin and blood [7]. Histologically, PG is characterized by a dense capillary network embedded within an edematous and inflamed stroma. Its external appearance may raise suspicion for malignancy, potentially leading to a misdiagnosis as a malignant lesion [1,2]. In a previous study examining upper airway vascular lesions in 639 patients, PG was identified in 73 cases. The oral cavity was reported as the most common site, whereas nasal involvement was less frequent [7]. Another study evaluating tongue pathology identified PG as the most prevalent benign lesion among biopsies obtained from individuals with suspected malignancies in the oral cavity [8]. In a study by Puxeddu et al. involving 40 patients with nasal PG, the most frequently affected site was the anterior septum, followed by the nasal vestibule, inferior turbinate, middle turbinate, and uncinate process [6]. Similarly, a study analyzing the pathology of 540 patients who underwent surgery for nasal masses reported a PG prevalence of 0.9% [9]. A retrospective study of 38 PG cases found that the condition was twice as common in women as in men, suggesting that hormonal fluctuations and nasal trauma may contribute to its development. The septum was identified as the most frequent site of origin for nasal PG, with epistaxis being the primary reason for hospital presentation [5]. In the present case, the patient presented with two primary complaints: epistaxis and nasal obstruction. Additionally, the lesion’s size raised cosmetic concerns. PG occurring during pregnancy is referred to as pyogenic granuloma gravidarum (PGG). The prevalence of PGG ranges from 0.5% to 5%, with most cases developing in the final two to three months of pregnancy. In the majority of instances, lesions are small and regress spontaneously postpartum. PGG is associated with elevated estrogen and progesterone levels during pregnancy. It is hypothesized that hormonal imbalances may stimulate endothelial cell proliferation in the oral and nasal mucosa in response to local trauma. Additionally, a documented association exists between oral contraceptive use and an increased risk of PG. Progesterone has also been implicated in PG development due to its interaction with estrogen receptors [2,7]. In the present case, surgical excision was performed for a rapidly enlarging PGG that emerged during the third trimester and failed to regress after delivery. On computed tomography (CT), PG typically appears as a unilocular, non-calcified soft tissue mass. Magnetic resonance imaging (MRI) often reveals a thin peripheral halo that is hypointense or isointense on T1-weighted images and demonstrates a heterogeneous signal on T2-weighted images [10,11]. Given the patient’s recent delivery and the lesion’s location in the anterior third of the nasal passage, our preliminary diagnosis was PGG; therefore, imaging studies were not performed. Various treatment modalities for PG have been described in the literature, including surgical excision, diode laser therapy, cauterization, embolization, silver nitrate cauterization, cryotherapy, and topical therapy. For small lesions, topical beta-blockers and imiquimod may be considered; however, surgical excision remains the preferred treatment due to its low recurrence rate. Small lesions can typically be excised under local anesthesia, whereas cases with a high risk of bleeding may require transnasal endoscopic surgery following preoperative super-selective embolization. During pregnancy, treatment decisions are guided by gestational age and anticipated blood loss. Lesions that do not regress postpartum are generally treated after delivery[1-3,7]. Surgical excision is performed in the subperichondrial or subperiosteal plane, ensuring a margin of normal mucosa is preserved to minimize the risk of recurrence. In the present case, the PG was excised in the subperichondrial plane, with a margin of intact mucosa maintained as the surgical boundary. ConclusionIn cases of rapidly growing nasal masses during pregnancy, especially in the third trimester, causing nasal obstruction and epistaxis, pyogenic granuloma gravidarum, a benign proliferative lesion, should be considered. Patient Consent: Informed consent was obtained from the patient for the publication of this study. Conflict of Interest: The authors declare no conflict of interest in this study. Financial Support: No financial support was received from any institution or organization for this study. Informed ConsentReferences
|
|||||
| Keywords : Piyojenik granülom , Hemanjiyom , lobüler kapiller , gebelik | |||||


|