

Authors
|
|||||||||||
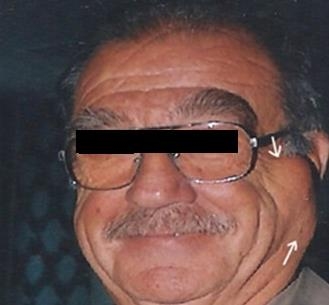
AbstractPleomorphic adenoma is the most common among all the tumors of the salivary glands. Deep lobe parotid tumors are relatively uncommon. We present a case of 67-year-old male patient with pleomorphic adenoma of parotid gland with an unusual extension of deep lobe origin, which underwent deep-lobe parotidectomy with preservation of the superficial lobe, successfully by surgeon.IntroductionPleomorphic adenoma (PA) is the most common among all the tumors of the salivary glands and accounting for 75- 85 % of all parotid gland tumours [1]. Symptoms, in most cases, the only sign is asymptomatic swelling that slowly grows in the parotid region without involving the facial nerve. The most of these tumors are between two and six centimetre. More than 90% of parotid tumours originate in the superficial lobe [2] but, approximately 10-12% of parotid gland tumors arise from the deep lobe, with only a small proportion (~1%) developing a significant parapharyngeal extension [3,4]. Pleomorphic adenomas of the deep-lobe present with a neck mass and when it is large, it may have an intraoral extension as well. It may also assume a dumb-bell shape as it enlarges and may be observed on Computed tomography (CT) or Magnetic Resonance Imaging (MRI) scans as prestyloid mass. Various modes of treatment have been advocated for benign parotid tumours ranging from enucleation to total parotidectomy [5]. Deep-lobe tumors have been managed mostly by a formal superficial parotidectomy and identification and preservation of the facial nerve, followed by removal of the deep lobe that contains the tumor [6]. In the present paper we presented a case of 67-year-old male patient with pleomorphic adenoma of parotid gland with an unusual extension of deep lobe origin, which underwent deep-lobe parotidectomy with preservation of the superficial lobe. Case ReportA 67-year-old male presented with a mass in the left parotid region, which had been present for about fourteen years. The patient did not complain of any associated symptoms. Physical examination showed a mass which was approximate 5x9 cm in size, of solid consistency, non-mobil, and not painful when palpated, was found in the left parotid region (Figure 1). His facial nerve was intact.
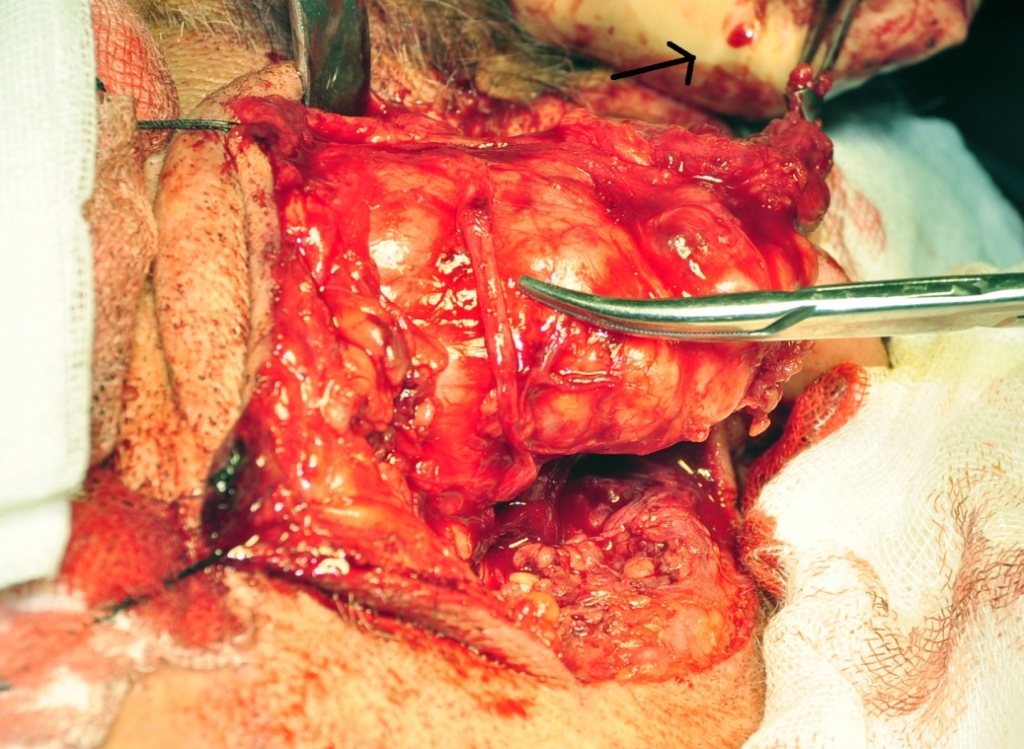
Magnetic resonance imaging (MRI) showed a large expansive oval mass, measuring about 6x4.5x2.7 mm in diameter, with apparently regular edges, in superficial parotid lobe. It showed a low-density in T1 and high-density in T2, evoking a solid formation. No lymphadenopaty was noted, and there was no significant enhancement of the mass following the administration of intravenous gadolinium-DTPA (diethylenetriamine-penta-acetic acid). After obtaining the patient’s inform consent to the surgical procedure, complete excision of the mass was performed using external approach. The critical point of the surgery was the localization of the facial nerve. The facial nerve was considerably pushed to infero-lateral of the parotid gland by the mass itself (Figure 2).
Following the facial nerve, the superficial lobe was dissected from the trunk to reach the mass which was completely located over and posterior edge of ramus and angulus mandibula. The upper limit of the mass extended to the root of the zygoma bone. The facial nerve was then gently dissected from the mass and the tumor was completely removed together with the parotid deep lobe (Figure 3).
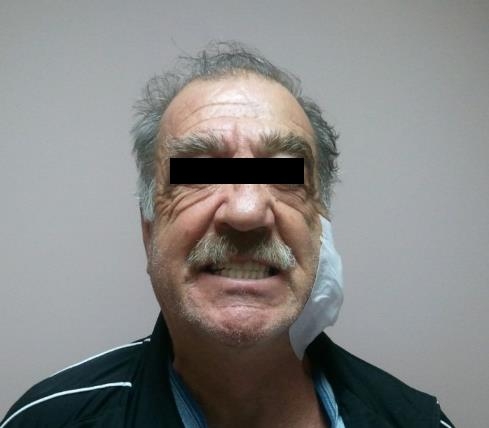
A large suction drain was left 4 days to make sure that the skin flap adherence was completed through the parotid bed. The patient was given intravenous cefazoline sodium postoperatively. Histological examination revealed a pleomorphic adenoma of the parotid gland. Facial nerve functions were intact postoperatively (Figure 4). The patient was regularly followed and there were no cases of tumour recurrence.
DiscussionPleomorphic adenoma is also known as ‘Mixed tumor’, which describes its pleomorphic appearance as opposed to its dual origin from epithelial and myoepithelial elements. PAs arises in patients in the fourth to sixth decade of life, with a female predominance. More than 90% parotid tumours originate in the superficial lobe [2]. Deep lobe parotid PAs are rare tumours. Aproximately 10-12% of PAs of the parotid are though to arise from the deep lobe of the parotid. These tumours have a variety of distinct clinical presentations, most commonly arising in the portion of the gland deep to the facial nerve yet lateral to the mandible, and present as pre-auricular masses. Isolated nodules are generally outgrowths of the main nodule rather than a multinodular presentation [3,5,6]. In our case, the parotid mass imitating the superficial lobe tumors and present as a pre-auricular mass, in examination. Computed tomography scanning or MRI depicts the mass, and the findings may essentially diagnostic in routine cases with typical features. MRI has the advantages of multiplanar imaging, and MRI results may suggest the tissue type on the basis of signal intensity characteristics. FNAC is mandatory to avoid any histological surprise. Open neck or trans-oral biopsies should be avoided, since opening the tumor capsule increases the risk of recurrence [1,3]. Deep lobe parotid tumours of various types should be removed by an external approach so that the facial nerve can be identified with precision and preserved if possible [7]. Temporary post-operative facial nerve weakness has been reported of 31% [8]. Ischemia of the nerve is thought to be the most important factor in causing this functional paralysis. Other factors include edema and stretching of the nerve, in particular of the finer branches [9]. Terrell at al. reported that use of facial nerve monitoring reduces the incidence of temporary facial nerve weakness post-operatively [10]. In our case, the facial nerve was thightened and its brunches were elongated because of the mass effect. Although this circumstance we did not observed facial paralysis or paresthesia in patient during follow up period. Total or near-total parotidectomy is a well- established technique for treatment of deep-lobe tumors, with the surgeon carrying out a superficial parotidectomy with preservation of the facial nerve followed by removal of the deep lobe that contains the tumor [6]. The ideal method excision would be to remove the tumor with a margin of normal tissue. Deep-lobe tumor capsule is very thick. Therefore less aggressive surgical approach is recommended and can rarely be excised with a complete covering of normal parotid tissue [11,12]. If initial surgical procedure does not completely remove the tumor, there is a low recurrence rate of less than 2%. Hussian A at al, suggested that deep-lobe parotidectomy is technically straight forward, it results in no postsurgical soft-tissue defect or asymmetry, and it provides an excellent aesthetic outcome [6]. In our case, despite preservation of the superficial lobe, there was more than adequate exposure of the deep lobe to execute surgery in a comfortable and safe way. There was no postsurgical volume defect and recurrence during the early follow-up period. Conclusion Deep lobe PA are rare benign tumors that are often clinically indistinguishable from lesion of the superficial lone of the parotid. The surgical approach should provide excellent visibility with wide surgical exposure to secure local neurovascular structures. References
|
|||||||||||
| Keywords : Pleomorfik adenom , Parotis bezi , Parotidektomi | |||||||||||



|