

Authors
|
|||||||
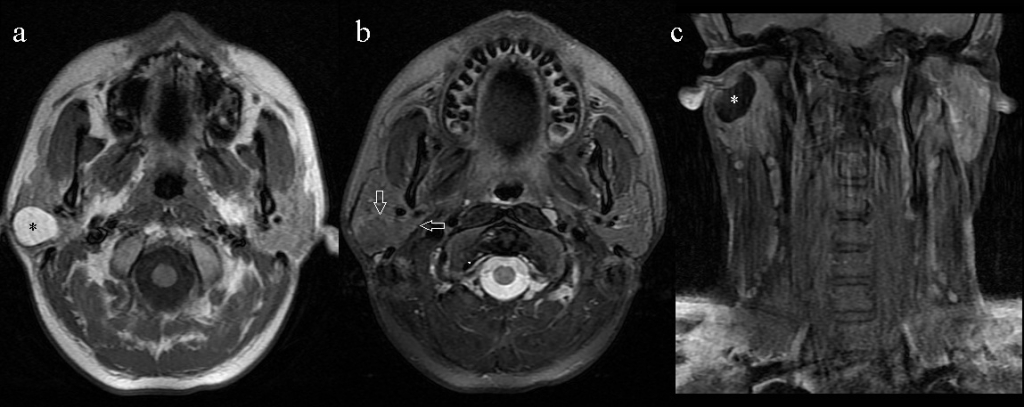
AbstractDermoid cysts of the head and neck are benign lesions and histologically composed of tissues originating from ectoderm and mesoderm. It is extremely rare in the parotid gland and should be considered in the differential diagnosis of a parotid mass. There are very few cases published in the literature. The treatment is surgical; despite its suggested to make superficial parotidectomy usually enucleation is sufficient. In this report we presented the diagnosis and management of a case operated because of a dermoid cyst in superficial parotid lobe.IntroductionDermoid cysts of the head and neck are benign lesions and histologically composed of tissues originating from ectoderm and mesoderm. These cysts can be congenital or acquired. Congenital cysts arise from a rest of embryonic epithelium. Acquired cysts are a result of traumatic implanted skin in deeper layers [1]. Dermoid cysts of the head and neck are uncommon and account for only 7% of all such cysts [2]. They are most often reported as arising in the floor of the mouth [3]. Dermoid cysts have only rarely been encountered in the parotid gland. A conclusive preoperative diagnosis may be difficult. Computed tomography (CT), magnetic resonance imaging (MRI), ultrasound and fine-needle aspiration cytology (FNAC) can be performed [4,5]. In this study, we presented a case with intraparotid dermoid cyst and discussed the diagnosis and treatment. Case ReportA 17-year-old man presented with swelling of the area of the right parotid gland for thirteen months. The patient was a non-smoker and had no further illness. Physical examination showed approximately 3 x 2 cm in diameter, soft, non-fluctuant mass in the right parotid gland. The patient showed no pain. Facial nerve function was normal. Pre-operative investigation included fine needle aspiration biopsy (FNAB), ultrasonography and magnetic resonance imaging (MRI). In the performed MRI, 26x16 mm round, well-defined, mass was identified in the superficial lobe of the right parotid gland which was hyper-intense on T1-weighted examination and hypo-intense on T2-weighted and fat-suppressed sequences, with no contrast uptake and no infiltration to surrounding tissue (Figure 1a, b, c).
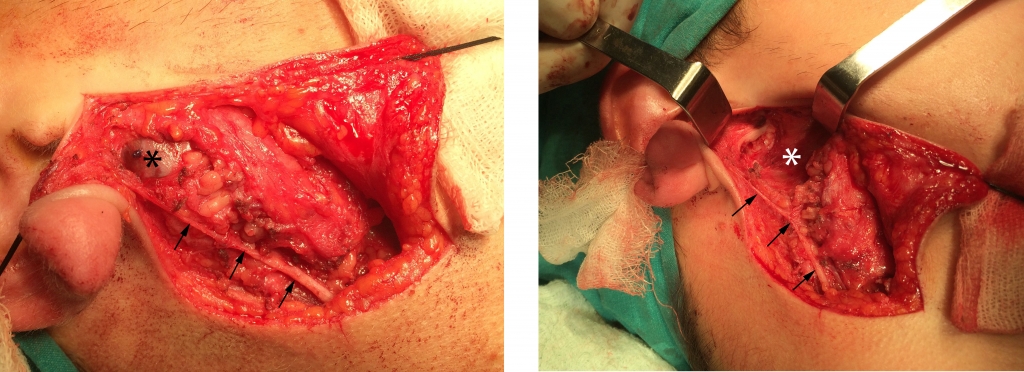
Ultrasonography (USG) showed untracked prominent anechoic cystic, 27x20 mm in size in superior portion of the parotid gland. Fine needle aspiration biopsy (FNAB) was performed and result of the cytological examination was reported as nonmalignant cells. Sialography was not performed. We planned parotidectomy under general anesthesia. The cystic mass localized in the right parotid superficial lobe was dissected from the surrounding tissue. Because the mass was connected to the tragal cartilage it is excised with the medial part of the tragal cartilage (Figure 2a, b).
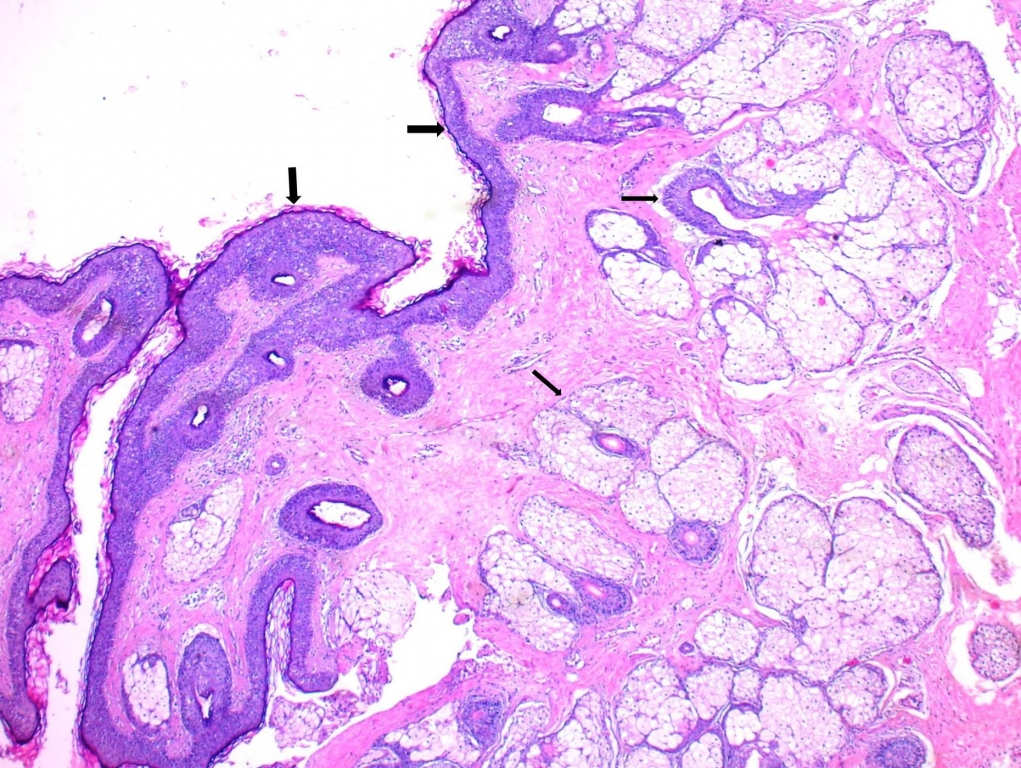
There was no connection with the external ear canal. The patient’s post-operative course was uneventful, with a normally functioning facial nerve evident at day one. The mass was cystic, encapsulated and filled with keratinous material macroscopically and the histopathological examination demonstrated a cystic structure lined by keratinized stratified squamous epithelium and units embedded in the cyst wall (Figure 3).
DiscussionThe dermoid cyst is a rare, congenital, epithelially lined, cystic cavity that contains tissues of both mesodermal and ectodermal origin. It may include skin and a variety of adnexal structures such as hair follicles and sebaceous glands. Most dermoid cysts in the head and neck region occur around the orbital, oral and nasal regions (80%); of these orbit tumors involve 49.5%, nasal tumors 12.6%, submental and submaxillary dermoids account for 23% and the remainder 14.6% [2]. Dermoid cysts are prone to form in these locations because they are the fusion sites of many embryonic structures [6]. Dermoid cyst occurring within the parotid gland is very rare. The large number of possible diagnoses of swellings of the parotid region and the fact that the clinical and radiological appearance is often ambiguous make a conclusive preoperative diagnosis difficult. The differential diagnosis includes mucous retention cyst, unilateral blockage of the parotid duct, benign mesenchymal tumors like lipoma, fibroma, hemangioma or neurofibroma, branchial cleft cyst, benign salivary gland tumors like pleomorphic adenoma, Warthin’s tumor and malignant salivary gland tumor like muco-epidermoid tumor [3, 6]. Ultrasonography, CT, MRI, and FNAB can be performed. Ultrasound may be helpful in differentiating between solid, vascular and cystic lesions [7]. MRI and CT may give an idea about the placement of the mass and relations with the surrounding tissue. CT will reveal a well-defined hypodense mass within the parotid gland. A content of fatty sebum would explain the diagnosis of lipoma suggested by MRI. Baschinsky et al. and Islam and Hoffman reported that the “anucleate squames” in the proteinaceous aspirate taken with FNAB supports highly the parotid gland dermoid cyst [4, 6]. The final diagnosis cannot be established until histopathological study of the surgical sample has been performed. Treatment of the dermoid cysts is surgical excision. Dermoid cysts are usually well encapsulated and this facilitates dissection. Superficial parotidectomy has been performed for treatment of the parotid dermoid cyst in the literature [6, 9-11]. No recurrence is reported of any of these cases. In the present case we did not perform superficial parotidectomy. During the operation considering the radiological and clinical features and the result of FNAB the cyst was totally excised with a piece of tragal cartilage by pericapsular dissection from the surrounding parotid gland tissue. There has been no recurrence in our patient at the time of writing (1.5 years). Malignant transformation of dermoid cysts has been reported at other locations with a probability of 5% [8]. Dermoid cyst is extremely rare in the parotid gland and should be considered in the differential diagnosis of a parotid cystic mass. There are very few cases published in the literature. The treatment of these cysts is surgical and enucleation is sufficient. References
|
|||||||
| Keywords : Dermoid kist , Parotis bezi , Neoplazm | |||||||

|