

|
|||||||||||||
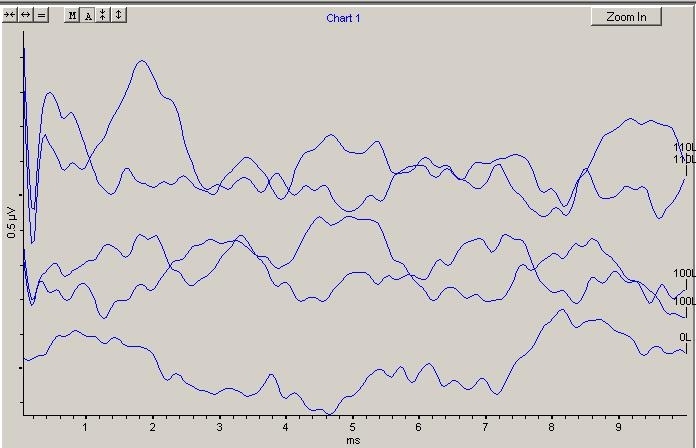
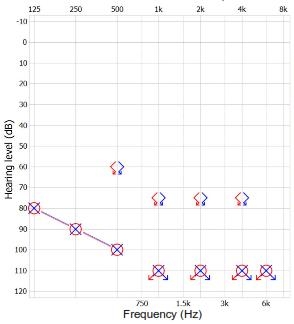
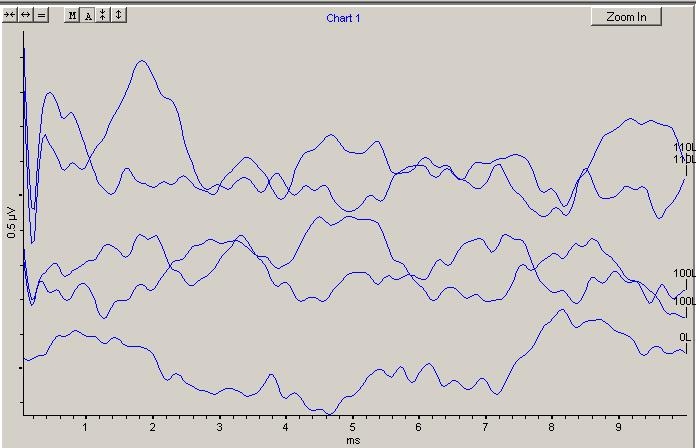
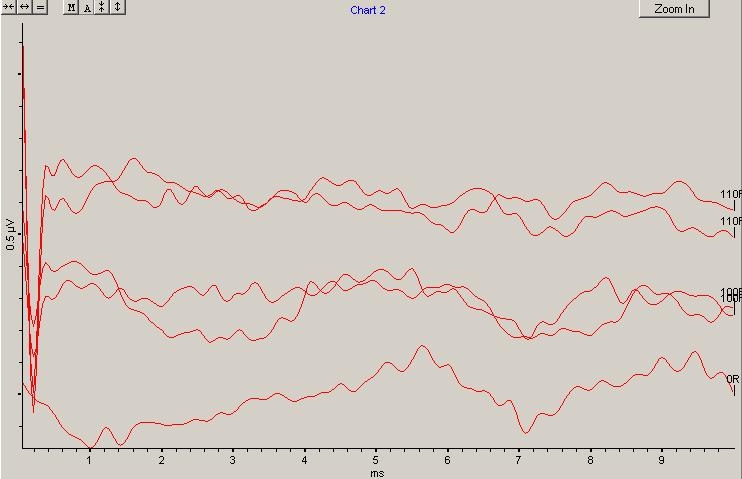
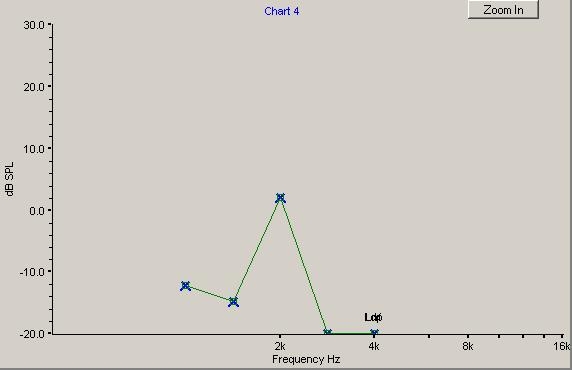
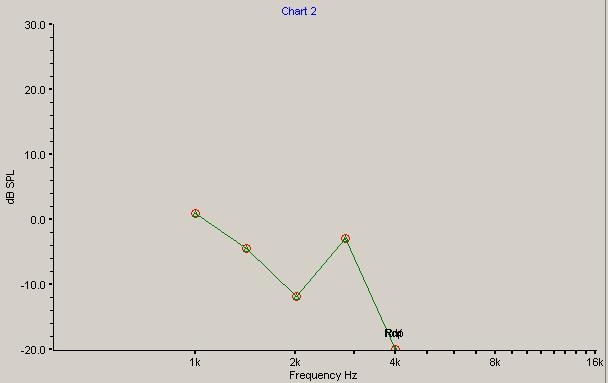
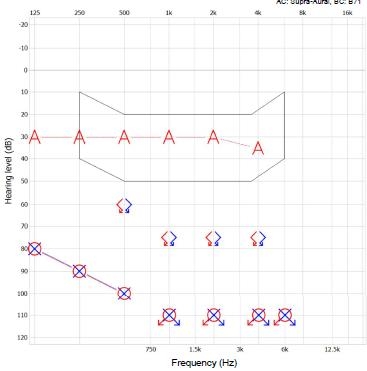
AbstractOtotoxic side effects of many antineoplastic agents and antibiotics have been reported, but there is not enough evidence about isoniaside. İsoniaside’s ototoxic side effect is mostly associated with end stage renal failure. There is no much way except to cessation of ototoxic drug when ototoxic effects are seen. Cochlear implantation is an important salvage option in bilateral sensorineural hearing loss. We are reporting a patient who was developed sensorineural hearing loss and bilateral visual loss during anti-tuberculosis treatment. The last chance for communication was cochlear implantation and it was performed with a successful outcome.IntroductionSensorineural hearing loss (SNHL) is a serious problem in using ototoxic drugs. Over 100 classes of drugs have been reported which have ototoxic side effects like hearing loss, tinnitus, dizziness and vertigo [1]. Aminoglycosides, antineoplastic agents, salicylates, loop diuretics are the most known Ototoxicity is generally associated with bilateral high-frequency SNHL [2]. Ototoxic SNHL may be temporary or permanent, slight or profound. It is generally irreversible and bilaterally symmetrical, and may occur even after single dose or may not manifest despite several months of therapy. Most of the antituberculosis drugs have neurological and toxic side-effects [1]. Streptomycin is one of these drugs with well known ototoxicity. Isoniaside is an antituberculosis drug and its variable neuropsychiatric effects are well known but there are not enough evidences about its ototoxic effects. Isoniaside associated sensorineural hearing loss has been reported rarely in end-stage renal failure patients (ESRF) undergoing hemodialysis. These adverse effects are usually seen during antituberculosis treatment. Impaired liver or renal function can lead adverse effects by the way of impaired drug metabolism. In this situation, there is no much way except cessation or stopping the drugs. Hearing aids or recently for profound hearing loss cochlear implantation is the treatment options. Here we present a patient who developed bilateral profound hearing loss and optic neuropathy during antituberculosis therapy and discuss cochlear implantation for this blind and deaf patient. Case ReportA 41 years old blind man was admitted to our clinic with bilateral SNHL. He was on hemodialysis program three times in a week for 13 years because of ESRF. He had a history of tuberculosis treatment one year and six months ago. He was administered quartet therapy including isoniazid 300 mg/day, rifampicin 600 mg/day, morphazinamide 1500 mg/thrice weekly and etambutol 1500 mg/ thrice weekly. He started to complain of vision loss 19[th] day of therapy and etambutol was stopped. Even etambutol was withdrawn, his vision declined and he became total blind. Hearing loss was started at 40[th] day of therapy. Hearing loss progressed even though cessation isoniaside and he had profound hearing loss. In neurologic examination, he had bilateral SNHL and bilateral total blindness. Routine laboratory tests indicated anemia, high urea and creatinine levels. His anti HCV level was positive. SNHL was documented by pure-tone audiometric examination (Figure 1). Fifth wave in auditory brainstem response (ABR) couldn’t be observed at 95 decibels (Figure 2). Bilateral otoacoustic emissions (OAE) were negative (Figure 3).
Cochlear implant was performed after 18 month of deafness and his audiologic performance was improved (Figure 4).
DiscussionPermanent hearing loss or balance disorders are serious complication of anti-tuberculosis treatment. İsoniaside, rifampin, pyrazinamide, etambutol, streptomycin are generally used drugs in tuberculosis treatment. Ethambutol’s most known adverse effect is retrobulber neuritis. Rifampicin’s most known adverse effects are hepatotoxicity, fever, thrombotic thrombocytopenic purpura, immune reaction results acute renal failure. Morphazinamide’s adverse effects are serious hepatic failure and renal failure. Streptomycin is an aminoglycoside drug and the most known ototoxic antibiotic. Streptomycin’s ototoxic effects (tinnitus, vertigo, deafness) are well-known. İsoniaside’s peripheric neuropathy effects, optic neuritis, encephalopathy, ataxia, disartria, depression, anxiety, schizophrenic psychosis are well-known adverse effects. In spite of all of them, there is not enough evidence about isoniaside’s ototoxicity. These adverse effects’ pathophysiologic mechanism is depending on pyridoxine deficiency. Isoniazid inhibits phosphorilation of pyridoxine and as a result decreases pridoxol-5-phosphate. Pridoxol-5-phosphate is a co-factor and neurotransmitter in many metabolic pathways. Because of ototoxic side effects, baseline audiologic tests should be obtained before the start of therapy. Baseline tests should include bilateral pure-tone air conduction threshold at standard audiometric frequencies from 0.25 to 8 kHz. If audiologic monitor allows, threshold frequencies above 8 kHz should be measured. Otoacoustic emission (OAE), auditory brainstem response testing (ABR) and Echo G should be obtained to from patients who are uncooperative to standard tests. Monitoring should continue regularly during therapy [3]. If there is no sign of ototoxicity, monitoring should be done weekly. SNHL is generally irreversible. Preventing and early diagnosing are more important than treatment. During therapy, using vitamin E, alpha lipoic acid or ginkgo biloba may be preventing ototoxicity. When hearing loss occurs, ototoxic agent should be stopped immediately. When hearing loss occurs, hearing aids can be used. Hyperbaric oxygen therapy may be helpful, but there is not enough evidence about it. If SNHL is bilateral and profound, cochlear implantation may be another treatment option. If a patient have renal insufficiency, preexisting hearing problems or a familial history of ototoxicity; ototoxicity risk may increase. Drugs’ ototoxic adverse effects are higher in end stage renal failure patients than normal population. Its pathophysiologic mechanism is probably associated with uremic toxins, ototoxins, and axonal uremic neuropathy [4]. The incidence of tuberculosis is increased in ESRF patients and side effects of antituberculosis drugs are more frequently seen in these patients [4]. Ototoxicity during antituberculosis therapy was reported in seven of 42 ESRF patients undergoing hemodialysis [5]. The administered therapy was not including streptomycin for all 7 patients. After stopping isoniaside in 4 patients, there was improvement of hearing loss in 2 patients, stable finding in 1 patient and progression in 1 patient. Our patient was administered quartet antitubercolosis therapy including isoniazid, etambutol, morphosinamide and rifampicin. On 19[th] day of therapy blindness was developed and on 40[th] day of therapy deafness was developed. Hearing and vision are the most important senses for communication, social life and education. There is nothing to improve vision but hearing aids are an option for hearing loss. If hearing aids don’t improve hearing cochlear implantation would be a good option. In this postlingual patient, hearing after cochlear implantation will be the most helpful sense for communication. We suggest that isoniaside ototoxicity could be seen in ESRF patients due to combined different neurologic effects. This group of patients should be monitored for hearing loss even streptomycin is not included to drug combination.
Abbreviations: ABR: Auditory Brainstem Responses ESRF: End Stage Renal Failure OAE: Otoacoustic Emission SNHL: Sensorineural Hearing Loss References
Presented at31. Türk Ulusal Kulak Burun Boğaz ve Baş Boyun Cerrahisi Kongresi. 29 Ekim-1Kasım 2009, Antalya/Türkiye |
|||||||||||||
| Keywords : Ototoksik yan etki , Sensorineural işitme kaybı , Koklear implantasyon , Geç dönem böbrek yetmezliği | |||||||||||||
|