

Authors
|
|||||||||||||
AbstractAlthough regional flaps are considered the first choice in midfacial and nasal tissue defects, the free radial forearm flap remains one of the superior options in larger defects. In this brief report, we present a unique case of a squamous cell carcinoma tumor originating from the columella and destructing the anterior nasal septum, the interior of the nasal dorsum, and the mid-upper lip. After resecting the lesion, a large composite defect was created. In order to achieve an acceptable functional and esthetic result, the defect was reconstructed with a novel designed free radial forearm flap + L strut bipartite vascularized radial bone. The radial bone was harvested based on two separate pedicles originating from the radial artery and concomitant veins. Afterwards, the bone flap was used to reconstruct the nasal septum, whereas the radial forearm flap was used to reconstruct new columella, nasal dorsum, and mid-upper lip structures in a composite fashion. As a result, the report describes a novel design of the free radial forearm flap and vascularized radial bone used in reconstructing a complex three-dimensional defect in the mid-facial region.IntroductionSince its description as a free flap, the radial forearm flap has been utilized in numerous modifications for reconstructing complicated tissue defects in the head and neck region [1,2,3]. In return, due to its pedicle length, skin paddle pliability, and vascular pattern, the radial forearm osteocutaneous free flap is considered a marvelous technique for oro-mandibular and maxillofacial reconstruction in certain well-defined circumstances [4,5,6]. Squamous cell carcinoma of the nasal columella (SCCNC) is an uncommon disease. The progression of advanced lesions is hard to manage and the prognosis is often poor. Such lesions indeed require a wide safe margin resection in return [7]. This report, describes a squamous cell carcinoma tumor originating from the columella invading the anterior nasal septum, interior of the nasal dorsum, and the mid-upper lip which was treated with a wide surgical resection and reconstructed with a novel designed free radial forearm flap and L strut bipartite vascularized radial bone. Case ReportA 53-year-old man was admitted with complaints of a non-healing ulcer on his nose. Physical examination revealed an ulserovegetative mass that was spanning the columella, the anterior nasal septum, and the upper lip (Figure 1).
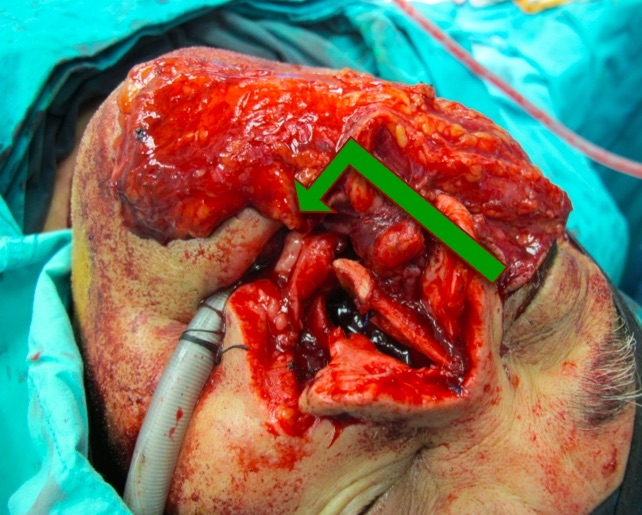
In the rhinoscopic examination, a mass was oblitaring both of the nasal passages. On the axial and coronal section MRI of the maxillofacial region, a 3.2x3x2.6 cm tumor was observed that extended from the columella to the cartilagenous septum and obliterating both of the nasal passages. The result of the insicional biopsy was reported as well-differentiated squamous cell carcinoma. Surgical Technique After obtaining informed conset from the patient a radical resection with immediate reconstruction was planned in one session. The bilateral supraomohyoid neck dissection was proceeded with a tumor resection at a 1-cm safety margin. An extensive defect that included the columella, all quadranguler cartilages of the septum, the entire tissue of the nasal tip, and the upper lip was created (Figure 2).
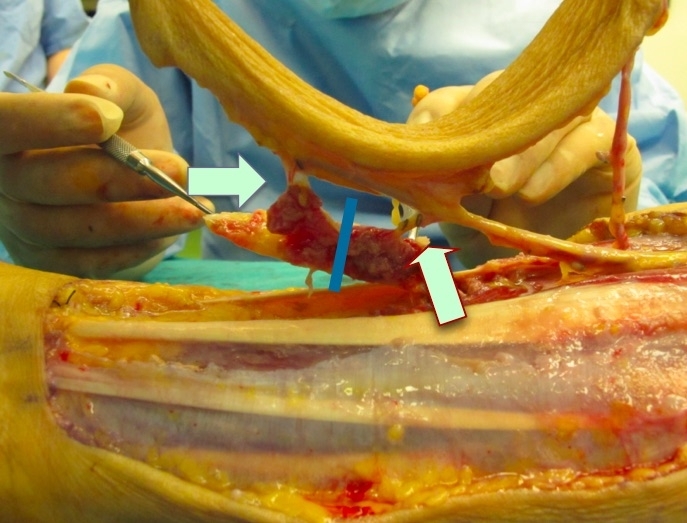
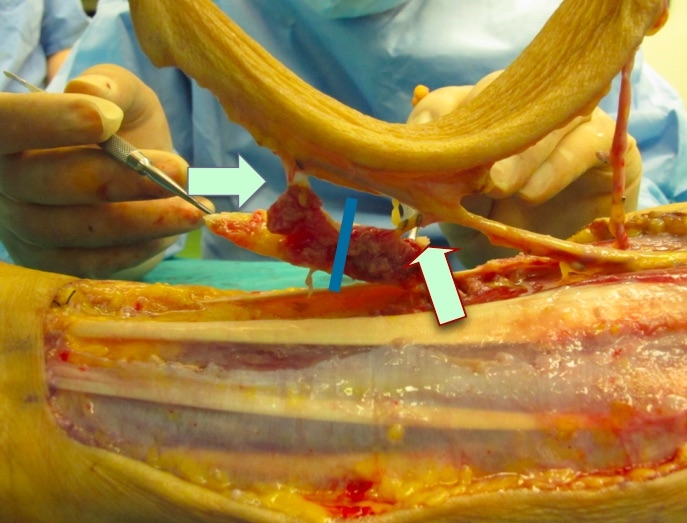
The radial forearm flap with a segment of the radius bone was harvested to reconstruct the upper lip and the nose defect, respectively. The flap was raised with an osseos portion from the radius nourished by two perforators (Figure 3 ).
The bone was split according to the vascular pattern in a bipartite fashion. Afterwards, the two boney segments were oriented in the L-strut to create a supportive structure in the mid-nasal part in the absence of the nasal septum. The nasal skin and the upper lip defect were reconstructed by tailoring the fasciocutaneous portion of the flap (Figure 4).
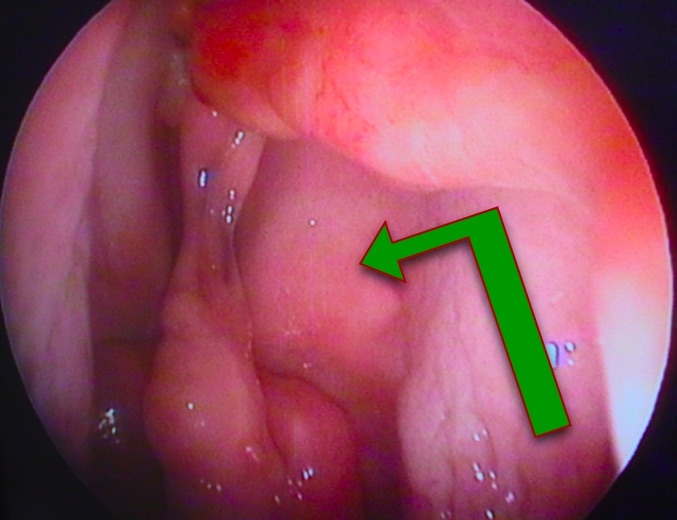
The facial artery and commitant vein were prepared as recipient vessels, and the left radial forearm flap based on the radial artery and cephalic vein was elevated with a marginal radius based on two perforators of the radial artery. Afterwards, the bone was split into two parts to create an L-strut to be adapted as a supporting nasal structure. The segments were fixed to the remaining maxillary spine and the perpendicular part of the ethmoid bone with 3/0 monofilament nonabsorbable sutures (Ethicon Inc., Somerville, NJ). Afterwards, the radial artery was anastomosed to the right facial artery, and the cephalic vein anastomosed to the right facial vein using 10/0 monofilament nonabsorbable sutures (Ethicon Inc., Somerville, NJ) The distal part of the radial forearm flap was adapted to the nasal edge of the skin defect, and the proximal part of the flap was adapted to the upper lip edge of the skin defect. To support the nasal airway passage, two silicone internal nasal splints (Invotec Inc, Jacksonville, Florida) were applied. The donor side was reconstructed with a split thickness skin graft. In the follow-up periods of six months, one year, and two years, no tumor recurrence was observed. As for the reconstructed nasal vault, the height created by the L-strut enabled a persistant nasal passage, which was observed with nasal endoscopic examination with a Storz telescope 0[°] (Karl Storz, Tuttlingen, Germany) (Figure 5).
Six months postoperatively the patient's external appearance was regarded acceptable (Figure 6).
DiscussionSeventy-five percent of nonmelanoma skin cancers are seen in the head and neck area, and 30 percent of these malignancies occur on the nose; however, lesions originating from the columella have rarely been reported [8]. Indeed, primary closure and full-thickness skin grafts are considered the first option for reconstructing relatively small and single layer nasal defects. As for larger defects, local regional flaps could be used as well [8]. Local flaps are actually indicated for proximal, middle, and distally located defects; bilobed flaps for nasal tip defects; and nasolabial flaps for nasal alar defects [8]. Paramedian forehead flaps are most preferred flaps for defects including more than one unit [8]. On the other hand, larger defects can be reconstructed combining forehead and nasolabial flaps. Defects involving the nasal cartilage lead to the loss of the nasal architecture. Morever, they may lead to a loss of function as well. Septal, auriculare, and rib cartilage can be used for the reconstruction of the nasal skeletal framework [8]. The reconstruction of full-thickness nasal defects need adequate replacement of the internal lining, skeletal support, and external cover [4,5]. In addition, the reconstruction of the inner lining in total rhinectomy defects is more difficult since a lack of nasal subunit tissues makes turn-in, septal, or sidewall mucosal rotation flaps unvailable. In such large defects, a free radial forearm flap can particularly stand out as a reliable vascularized tissue. Midfacial defects ( perioral and nasomaxillar areas ) are not usually seen. And also it is hard to reconstruct because of complicated characteristics of the area. There are various alternatives that can be applied to those extensive defects, such as prosthetic devices, osseointegrated implants, pedicled flaps with the aid of autologous or alloplastic grafts, and microvascular free flaps [9]. Staged procedures have been more useful for midfacial reconstruction using a prosthetic device, a distant flap, and one or multiple autologous free flaps. However, these staged techniques require a prolonged operation time and may cause serious problems, such as wound infection, psychiatric problems, scarring from a nonfunctional upper lip, the contraction of free flaps, and weak support of the palate. In one report, three free flaps were used to reconstruct a middle and lower facial defect in a single stage, which provided better aesthetic and functional outcomes, preventing the contraction of the remaining facial soft tissues [10]. On the other hand, in the presenting report, the chimeric nature of the flap might have provided additional tissue such as bone, without the need to harvest tissue from another donor area. For the reconstruction of complex midface defects, particularly those that are full thickness, radial forearm flap is considered to be a good selection. One advantage of this flap is that it can include the radius if necessary. Although the radial forearm is probably one of the most pliable and thin flaps amenable to vascularized transfer, it is still bulky compared to normal nasal mucosa. This flap requires extensive subsequent thinning and contouring in the second stage of reconstruction. The patients required regular nasal irrigation because of the loss of normal nasal ciliated tissue and because of the presence of a keratin-producing epithelium in the nasal cavity. Moolenburgh developed an algorithm after reviewing 788 patients files and literature [8]. The author divided nasal defects into simple, small (skin only), larger (skin and cartilage), or full thickness. Small defects can be closed by primary or various local flaps. Larger defects can be closed by the forehead flap with or without the use of cartilage grafts. Small inner lining defects can be closed by full-thickness skin grafts or turn-down lining flaps with delayed primary cartilage grafts. For medium to larger inner-lining defects, the folded forehead flap can be closed with cartilage grafts. With very large inner-lining requirements, free vascularized tissue transfer would be a better choice. In certain conditions, as in this particular case, reconstruction with a composite flap might have been an good option since the defect included both the nasal structures and the upper lip. Although adding a forehead flap to the reconstructed area would have provided a better cosmetic result, the patient refused to take the additional option. The segmental vascularity of the radius in relation to the radial artery was principly utilized to create a vital L-strut support. In addition, integrating the vascularized bone into the radial forearm flap resulted in a flap with different types of tissues to be addressed for three-dimensional reconstruction. In conclusion, this technique could provide a composite tissue that can be a good substitute for the other multiple-flap option. References
Presented atOral Presentation: 7. National Rhinology Congress (19-22 May 2011, Belek-Antalya ) |
|||||||||||||
| Keywords : Vasülarize L-strut , Radial ön kol flebi , Orta yüz | |||||||||||||



|