

Authors
|
|||||||||||||||||||
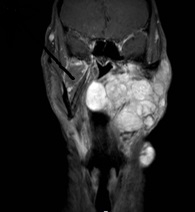
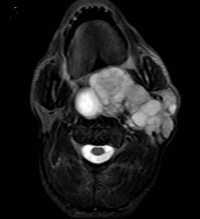
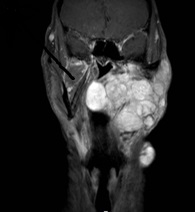
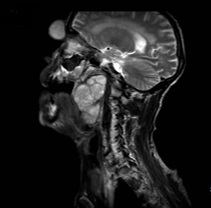
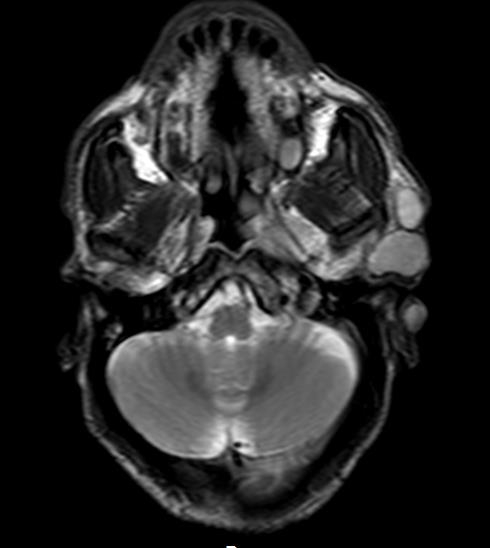
AbstractCarcinoma ex pleomorphic adenoma is a rare tumor that results from the carcinomatous transformation of a primer or recurrent pleomorphic adenoma. A 75-year-old male patient presented with a solid mass in his neck and respiratory failure. The patient had a 20-year history of this disease. A clinical examination revealed a solid and fixed mass with a number of lobules that fully pervaded the 2nd region on the left side of the neck, arising from the left parotid. Facial nerve functions were good. Furthermore, solid and mobile masses were identified in the frontal region, below the scalp, in the auricle of the left ear and the in left superficial layer of the sternocleidomastoid muscle. An oropharynx examination revealed that the left tonsil region had passed to the midline of the neck, pushing the uvula under the effect of the mass. In an MRI of the neck, the image involved the masticatory and parapharyngeal area that filled in the left parotid on the skull base, narrowed the Rosenmuller fossa on the left superior and obliterated significantly the air lumen on the oropharynx level. The mass extended to the hyoid bone in the caudal and to the bottom of skin-to-skin in parotid region. The measurable size of the mass was 9 x 10 cm. The patient underwent a total parotidectomy and a left neck dissection in surgery, and in addition, other masses in the neck and the head were excised.IntroductionSalivary gland neoplasms constitute 3–4 percent of all head and neck tumors, affecting around 2.5-3/100,000 people each year [1]. Pleomorphic adenomas are the most commonly found tumors among salivary gland tumors, with 90 percent located in the parotid with a superficial lobe origin, and 10 percent with a deep lobe origin [2]. After surgical treatment, pleomorphic adenomas may reoccur between 1–46 years later. The malignant transformation of such tumors is a rare condition, occurring in only 3–4 percent of cases. The malign type, known as carcinoma ex pleomorphic adenoma is frequently observed in long-term or recurrent cases [3]. Less than 2 percent of pleomorphic adenoma cases may be histologically presented with a benign but clinically and highly malignant table [4], and in these cases, bone, liver, lung and regional lymphatic metastases have also been reported, as well as the local aggressive progress [5]. In our case, the carcinoma ex pleomorphic adenoma had existed for a long time and had grown to a very large size, leading to ocal metastasis in head and neck region, and is presented and discussed in this paper with reference to previous literature. Case ReportA 75-year-old male patient was admitted with a hard mass in the neck, and suffering from respiratory failure. The patient had a 20-year history of this disease. A clinical examination revealed a solid fixed mass with a number of lobules that fully pervaded the 2[nd ]region on the left side of the neck, arising from the left parotid. Facial nerve function was good. Furthermore, solid and mobile masses were identified in the left superficial layer of the sternocleidomastoid muscle and the auricle of left ear under the scalp in the frontal region. During an oropharynx examination it was observed that the left tonsil region had passed to the midline of the neck, pushing the uvula under the effect of the mass. In an MRI of the neck, the image involved the masticatory and parapharyngeal area that filled in the left parotid on the skull base, narrowed the Rosenmuller fossa on the left superior and obliterated significantly the air lumen on the oropharynx level. The mass extended to the hyoid bone in the caudal and to the bottom of skin-to-skin in parotid region. The measurable size of the mass was 9 x 10 cm. In the MRI the T1 was mildly hyperintense and T2 was a hyperintense lobule-contoured contrast-enhancingsolid mass (Figure 1a,1b,1c,2,3).
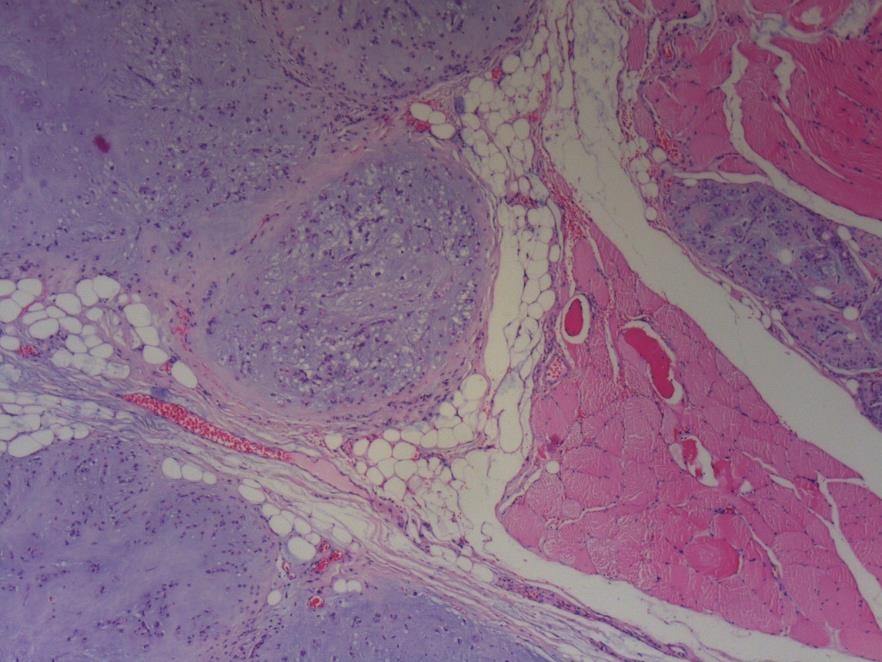
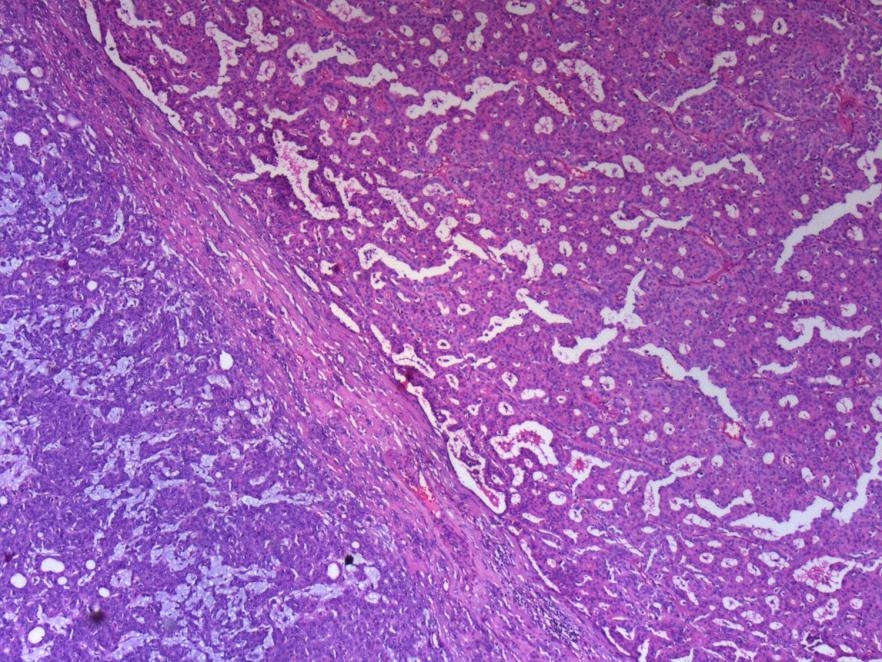
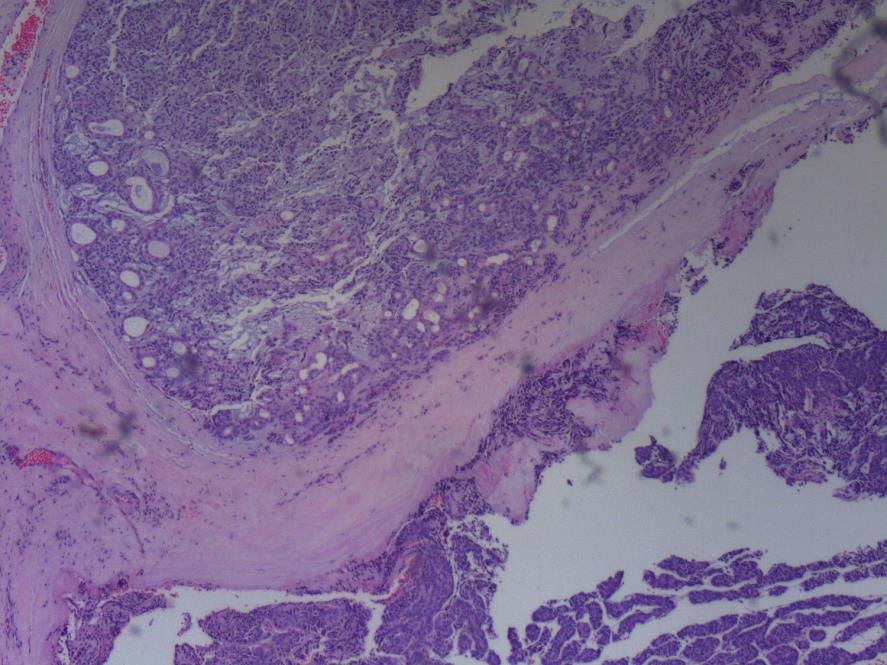
The patient underwent a total parotidectomy and a left neck dissection , during which other masses in the neck and the head were excised (Figure 4).
Written informed consent was obtained from the patient who participated in the study. DiscussionPleomorphic adenoma is the most common form of tumor in the parotid gland. Although its characterization is benign, its rate of recurrence is high. Tumors may spread to large areas such as the parapharyngeal space in patients with long-term complaints and in those with a late diagnosis. The potential risk of becoming malignant is 1–7 percent as an annual incidence [6]. Masses are usually determined in the neck upon physical examination, and the neck mass in the present study reached a large size. The mass of the patient extended into the parapharyngeal space, and was intraorally detected due to its large size. Large masses result in such complaints as difficulty in breathing and dysphagia in patients due to the resultant narrowing of the air passage in the oropharynx and nasopharynx. Furthermore, in the present study, mobile, smooth surfaced and solid masses were identified in the superficial of sternocleidomastoid muscle, in the ear auricle below the hairy skin, and under the scalp in the frontal region of the patient’s head and neck. Carcinoma ex pleomorphic adenoma is usually seen in women in the sixth and seventh decade of life, and occurs mostly in the parotid gland [7]. The malignant component of carcinoma ex pleomorphic adenoma is demonstrated through the exceeding of the capsule of the benign component, and this is suggestive of invasion and malignancy, raising the risk of metastasis into the regional lymph nodes [8]. Brandwein detected no recurrence or metastasis in tumors that invaded areas smaller than 1.5 mm [9]; although Felix A et al. presented a case in which a carcinoma ex pleomorphic adenoma had been completely encapsulated with regional metastases for 10 months after the onset of the disease [10]. In the present case, metastasis spread to the regional lymph nodes, and regional metastases were also identified in many areas below the skin and in the subcutaneous tissue of the head and neck. A review of literature indicates that such metastasis is uncommon. A prognosis of carcinoma ex pleomorphic adenoma depends on the degree of invasion and lymph node involvement, and pathological parameters such as local and distant metastases. A prognosis of non-invasive and minimally invasive carcinoma ex pleomorphic adenoma is better than one of invasive carcinoma ex pleomorphic adenoma. The size of the tumor and the level of invasive carcinoma ex pleomorphic adenoma are also important prognostic markers. A clinical prognosis of cancer depends on the carrying out of a complete tumor resection. In addition, a full and aggressive surgical and radiological treatment of carcinoma ex pleomorphic adenoma can increase survival rates in patients . The treatment of carcinoma ex pleomorphic adenoma varies according to its location, and involves a radical resective procedure. A superficial parotidectomy is applied in the case of non-invasive and minimally invasive carcinoma ex pleomorphic adenoma; and if there has been invasion into the surrounding tissues, a total parotidectomy is carried out. In case of cervical lymph node metastasis, a neck dissection should be performed . Generally, in the event of a perineural invasion, there are indications for radiotherapy in suspected surgical margin resection in the presence of pathologic lymph node in high-grade tumors . In summary, large tumors that are locally aggressive, and that lead to respiratory failure and cause multiple metastases (frontal region, left ear auricle, left superficial of sternocleidomastoid muscle, below the scalp) just below the surface of the skin in the head and neck region are rare. We believe that our case is very rare and will contribute to literature based on the different clinical picture of the patient. No sponsorships or competing interests have been disclosed for this article. References
Presented atPoster olarak Türk Ulusal Kulak Burun Boğaz ve Baş Boyun Cerrahisi 35.kongresi 2-6 Kasım 2013 te sunulmuştur. |
|||||||||||||||||||
| Keywords : Dev karsinoma ex pleomorfik adenom , Solunum sıkıntısı , Multiple metastaz | |||||||||||||||||||


|