

|
|||||||||||
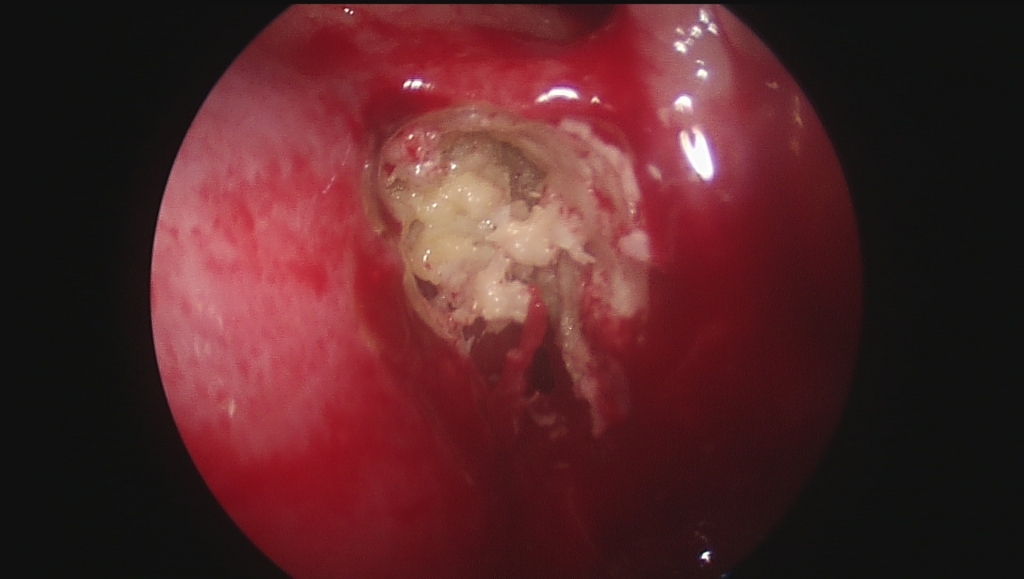
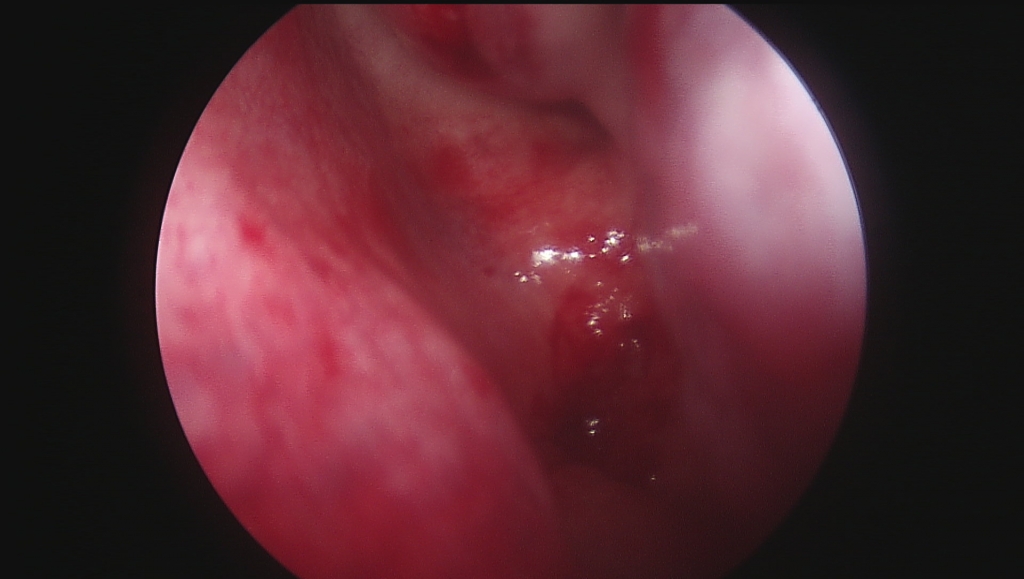
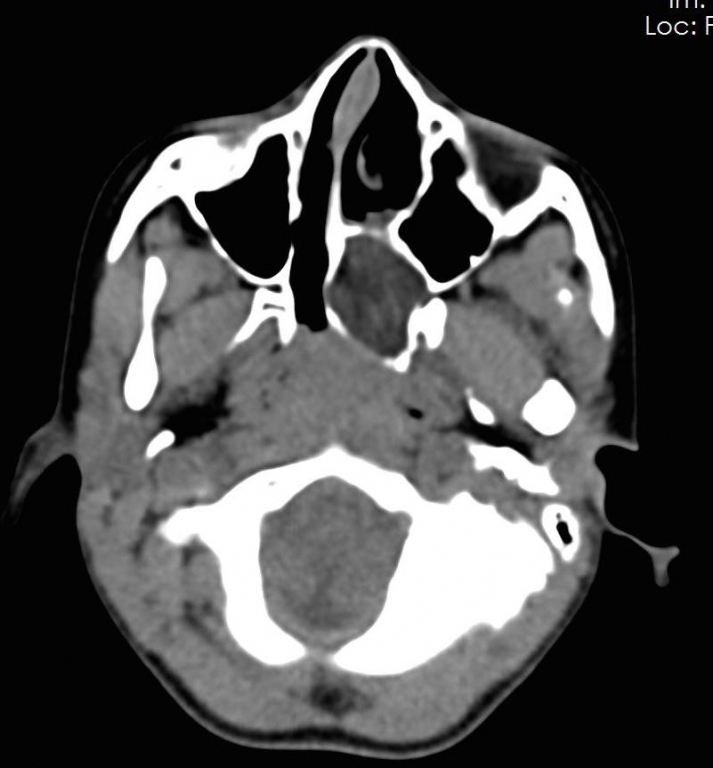
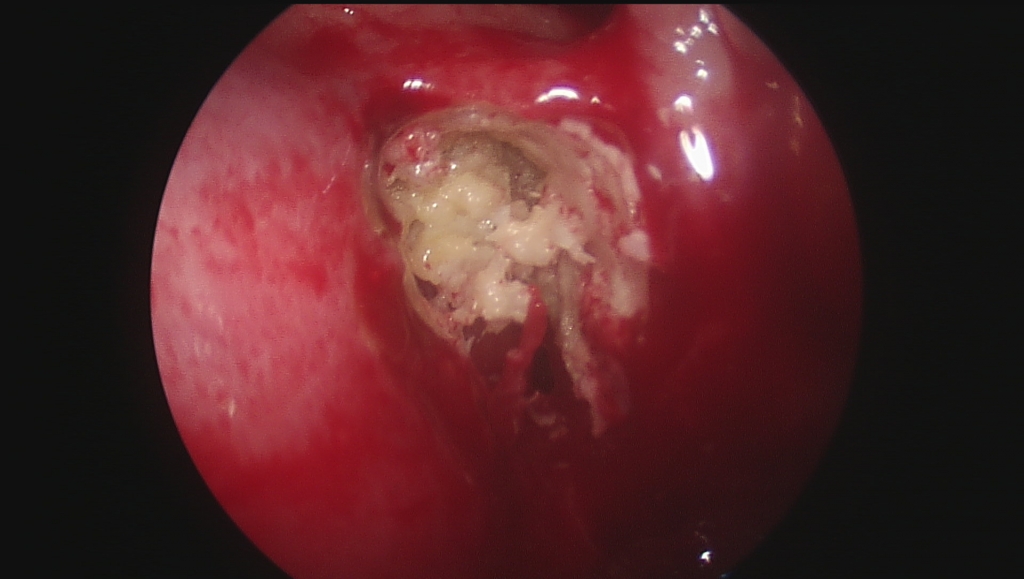
AbstractA nasal dermoid cyst is a rare developmental anomaly seen in children. There are many classification systems of dermoid cysts according to anatomic localisation or extent of the lesions. However, comprehensive classifications have not been reached.We have reported a case of a nasal dermoid cyst located in a bone capsule in the left nasal passage. This is an unusual localisation for these cysts, which usually occur at the anterior skull base. A full endoscopic resection of the left nasal dermoid cyst was successfully performed. There were no peri-operative complications. All classifications describeintraosseous nasal dermoid cysts at the anterior skull base, at the nasal bone. This is the first case report of an intraosseous nasal dermoid cyst located at the posterior nasal passage. The clinical features and successful endoscopic treatment of this unusual patient are presented in the literature. IntroductionA nasal dermoid cyst typically presents as a midline mass and may be located anywhere from the base of the columella, along the nasal dorsum, to the nasoglabellar region [5]. Congenital midline nasal masses occur in 1 out of 30,000-40,000 live births, and dermoid cystsconstitute the most common cause [1]. The term ‘nasal dermoid cyst’ was first described by Cruvelier in 1817 [2]. Nasal dermoid cysts account for 1%–3% of all dermoid cysts and approximately 4%–12% of head and neck dermoid cysts [3,4]. Pathogenesis involves an incomplete obliteration of neuroectoderm in the nasofrontal region. Congenital dermoid cysts contain only ectodermal and mesodermal embryonic elements such as hair follicles, sebaceous glands, and sweat glands. There is a strong debate on the classification of nasal dermoid cysts, and there is no clear classification that is accepted by all surgeons. Dermoid cysts have been sortedby many authors into four categories,based on inclusion sites [6]. Hartley et al. proposed a new classification according to the extent of the lesion [7]. Unfortunately, the classification system is not yetcompleted, since new cases on atypical localisation with unusual behaviour have been added to the literature. We are hereby presenting a dermoid cyst located in a bone capsule at the left posterior nasal passagewith its endoscopic treatment. This is the first paper to present an intraosseous nasal dermoid cyst located in the posterior nasal passage. Case ReportAn eight-year-old girl displayed halitosis and a nasal obstruction for three years. She had a history of intermittent nasal discharge but no history of nasal foreign bodies. On examination, the right nasal passage was open and clear. The flexible nasopharyngoscopy examination revealed adenoid tissue causinga 40% obstruction. A dense mucopurulent secretion was observed during the left nasal examination. When re-examined after an aspiration and decongestant treatment (Figure 1), the left nasal passage was completely obstructed at the posterior site. A computed tomography (CT)scan was performed, showing a 28x24 mm intraosseous soft-tissue density located between the sphenoid sinus and hard palate(Figure 2).
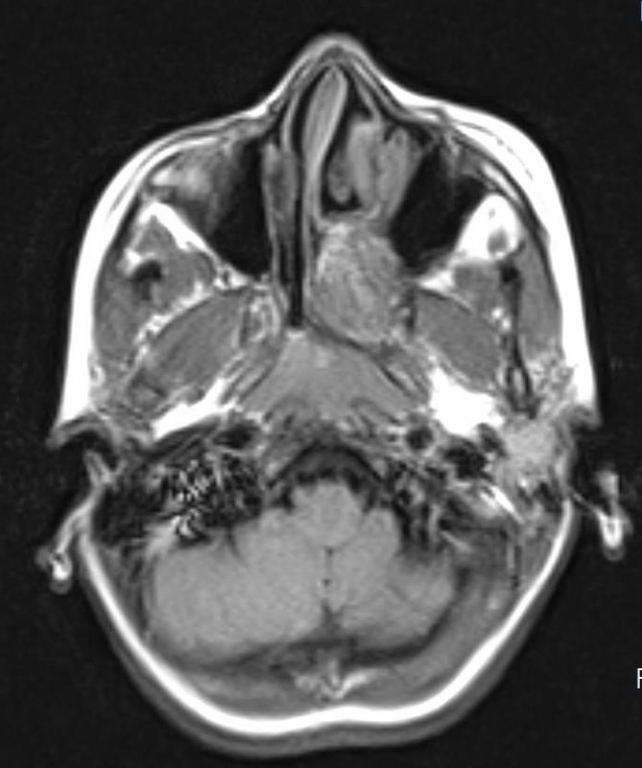
The mass was well-defined and expansive at the left nasal passage. There was no evidence of intracranial extension or dehiscence of the skull base. Amagnetic resonance imaging (MRI)presented a heterogeneous,intraosseous soft-tissue (fat-density) enhancement at the left nasal passage(Figure 3). The patient was otherwise healthy; the upper airway examination was normal. The imaging and the clinical features were consistent with a congenital nasal mass.
We informed the patient’s parents and decided on an endoscopic approach to the nasal mass, performed under orotracheal intubation. We used 0[0]and 45[0]4 mm rigid endoscopes for operation. A white caseous lesion was observed when the anterior site was opened with aKerrison punch (Figure 4).
The bone formation at the anterior site of mass was removed and mass-dissected from adjacent structures. All intraosseous soft tissue was removed with a curette. Bleeding control and nasal packing were performed when all the nasal mass was cleared. The patient was discharged a day after the operation. There were no peri-operative complications during the operation orpost-operative period. The nasal obstruction was resolved just after the operation. The definitive histopathological examination described a squamous epithelium with a fibroadipose stroma, consistent with a dermoid cyst. A follow-up at one week and one, three, and six months (with a nasal endoscopy and CT at the sixth month (Figure 5) did not show any evidence of persistence or recurrent disease.
DiscussionMost dermoid cysts areconfined to the nasal skin (61%), although they do extend to the nasal cartilage (16%), cribriform plate (12%), nasal bone (10%), and ethmoidal air cells (1%), as noted by Bradley [8]. These lesions might be associated with a sinus opening, intermittent discharge of sebaceous material,or recurrent infection. There are alsosomerare dermoid cysts located at the Eustachian tube or nasopharynx [9,10]. Classical patterns of Eustachian tube or nasopharyngeal dermoid cysts manifest as pedunculated or sessile polypoid structures that are usually free from adjacent structures. With its clinical and radiological results, our case waseasily differentiated from Eustachian tube or nasopharyngeal dermoid cysts. There are a few classifications of nasal dermoid cysts that addressclinical and radiologic features and depend on the localisation of the cysts. Hartley et al. proposed new classifications of nasal dermoid cysts according to the extent of the lesions: superficial, intraosseous, intracranial extradural, and intracranial intradural [6]. They arrangedthe cysts into four subgroups corresponding to clinical and imaging features. This classification describes an intraosseous dermoid cyst sub-group at the anterior skull base that extends into the nasal bone. In our case, there was a nasal dermoid cyst causing expansion at the nasal septum and lateral wall of the nasal passage, located between the anterior sites of the sphenoid sinuses and hard palate. This is an unusual location for nasal dermoid cysts that boundaries with bone formation at four site with mucosal lining. The standardlocalisation of intraosseous lesions is the anterior skull base, at the nasal or frontal bones. Our case displays unusual clinical and radiological features of nasal dermoid cysts compared to the literature. The definitive treatment of nasal dermoid cysts is surgical excision; in our case, the lesions were predominantly superficial and involved local excision and direct closure. Open rhinoplasty was also used either alone or combined with direct excision. Intraosseous lesions extended to the nasal and frontal bones and would require a bone drill for complete surgical excision. The intracranial extradural lesions breeched the anterior cranial vault and could be accessed via a limited frontonasal osteotomy and peeled from the dura. In addition, the intracranial lesions may be successfully excised and the skull base reconstructed endoscopically [11]. Endoscopic approaches are usuallyprioritized to remove Eustachian tube or nasopharyngeal dermoid cysts, since visualization of close vital structures is limited for complex anatomy. We also used an endoscopic approach to remove the mass for better visualization of small nasal structures. Our case involved an eight-year-old patient with nasal dermoid cyst. These were the characteristics of the cyst: cyst causing expansion at the nasal septum and lateral wall of the nasal passage, located between the anterior sites of the sphenoid sinuses and hard palate and boundaries with bone formation at four site with mucosal lining. It does not fit into typical classification because intraosseous dermoid cysts were defined into nasal bone. This is the first case report of a nasal dermoid cyst that has a bone capsule at the posterior nasal passage, and we contribute to the literature with this paper. References
|
|||||||||||
| Keywords : Nasal dermoid , Konjenital anomali , Orta hat nazal kitle , Pediatrik , Endoscopik rezeksiyon | |||||||||||

|