

|
|||
AbstractPeritonsillar abscess (PTA) in the absence of tonsil tissue is rare. Congenital branchial fistulas, Weber’s glands and dental disease are among the possible sources of infection. The consideration of these etiologies in cases of PTA formation with the absence of concurrent tonsillitis may effect management decisions.We report the youngest case of peritonsillar abscess in a tonsillectomized patient. The boy had undergone tonsillectomy and adenoidectomy at the age of three. He was diagnosed with Kawasaki disease a year before he presented to our clinic and had recovered with IVIG therapy. At the age of eight, he presented with odynophagia, trismus, malaise, decreased oral intake, pharyngotonsillar bulge, and limited neck motion. A CT scan was taken and revealed a homogenous hypodense abscess showing peripheral contrast involvement in the left parapharyngeal-peritonsiller space 2.7x1.6 cm in dimensions. The abscess responded to IV medical therapy with penicillin and metronidazole without necessitating drainage or surgical intervention. This case is the 12th and the youngest case reported in the literature. IntroductionPeritonsillar abscess (PTA) is a common otolaryngological emergency. Patients commonly present with unilateral sore throat, fever, trismus and decreased oral intake. In clinical examination, the tonsil is displaced medially with the displacement of the uvula to the contralateral side and swelling of the soft palate. PTA generally develops as a complication of acute tonsillitis when infection penetrates through the tonsil capsule where the pus is collected between the fibrous capsule of tonsil and the superior constrictor muscle of the pharynx. Nevertheless, the etiology is definitely more complicated as PTAs also arise in patients with no previous history of tonsillitis. Possible sources of infection can be congenital branchial fistulas, Weber’s glands and dental disease [1]. To date there have been 11 reported cases of PTA after tonsillectomy. The case presented in this paper is the 12[th] case and he is the youngest patient reported to date and the second pediatric case. This case is also the only case having a prior Kawasaki disease history. Therefore, we aimed to report this rare case, and discuss the potential etiology and anatomy of PTA formation and its relation to tonsillectomy. Case ReportAn 8-year-old boy was admitted to the department of pediatrics with malaise, trismus and decreased oral intake. The patient gave a history of severe left-sided throat pain lasting for ten days, associated with odynophagia, trismus, decreased oral intake, and limited neck motion. His symptoms had not improved despite treatment with oral antibiotics. There was no abnormality except for leucocytosis, neutrophilic dominance and elevated C-Reactive protein in laboratory. In his history, the boy was diagnosed with Kawasaki disease in another hospital one year before he presented to our clinic, and had recovered with IVIG therapy. He had had an uncomplicated tonsillectomy and adenoidectomy when he was three because of airway obstruction. In his physical examination, swelling of the left soft palate and displacement of uvula to the right was seen with no residual tonsil tissue. A computerized tomography (CT) scan was taken and revealed a homogenous hypodense abscess showing peripheral contrast involvement in the left parapharyngeal-peritonsiller space 2.7x1.6 cm in size. The left parapharyngeal fat planes were erased. No pathologic lymph nodes were observed. The patient was commenced on IV penicillin and metronidazole. The patient responded to antibiotherapy without necessitating drainage or surgical intervention. After the trismus, torticollis and palatal edema subsided, he was discharged home on oral antibiotics three days later. He was evaluated in clinic a week after discharge and the repeat examination showed no signs of infection, no evidence of remnant tonsil tissue and the laboratory findings were normal. He did not have a recurrence in 2 years.
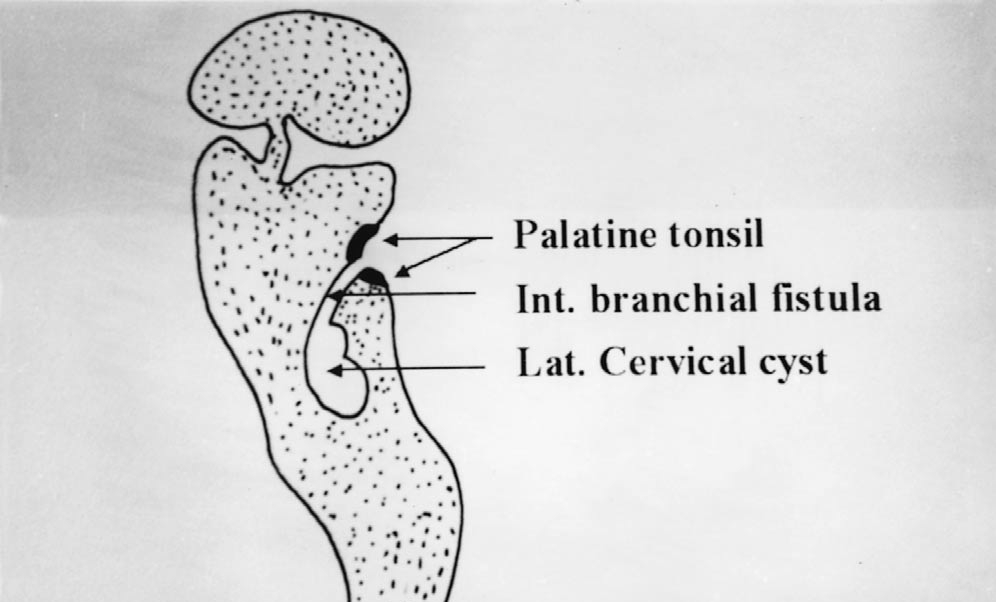
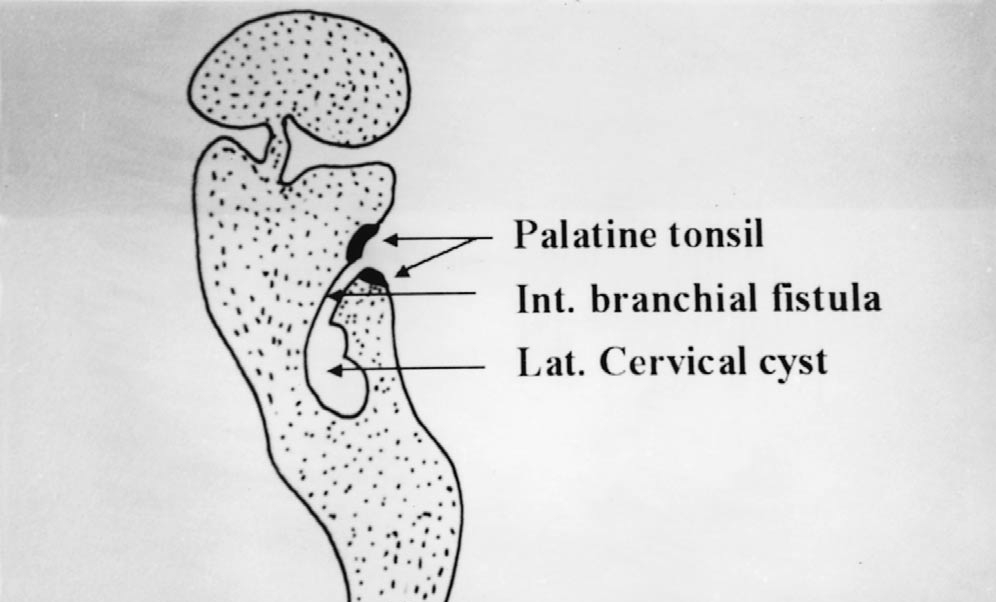
DiscussionPTA has been reported in patients who had undergone tonsillectomy [1,2,3]. Nevertheless, most of the cases reported in the literature are associated with tonsillar remnants providing a potential source of infection. However, in the 12 cases which are reported including ours, there is no sign of residual tonsil tissue. The reported case is also the youngest patient reported to date and the second pediatric case. The pathogenesis of PTA after tonsillectomy is still unclear and confusing, assuming tonsil tissue is removed and the peritonsillar space is obliterated. However, if the tonsil capsule is not entirely excised during the tonsillectomy, this can be an explanation for the development of a PTA in a superior location. Even when the tonsil capsule is entirely excised, suppuration may arise in any remnant peritonsillar tissue. Pus may be collected between the superior constrictor muscle and any fibrosis resulting from the tonsillectomy. If this is the case, the patient should be treated with needle aspiration of the affected area and antibiotics. Removal of the remaining tonsillar tissue and surgical capsule of the tonsil is also advocated [4]. Several other theories have also been implicated for the development of PTA after tonsillectomy. The tonsils are derived from the 2nd branchial pouch and occasionally the membrane between the pouch and cleft persists, which gives rise to an internal branchial cyst and fistula or both (Duct of His). The congenital anomaly lying between the tonsil and the superior pharyngeal constrictor muscle may persist as a cyst or fistula, and drain via a tract to the normal derivative of the 2nd branchial pouch, the tonsilar fossa. This may explain the occurrence of PTA in the absence of a tonsillar infection. If there is a potential cyst or fistula, tonsillectomy may even predispose to recurrent abscess, when the post tonsillectomy scar tissue obstructs the drainage of the cyst or fistula tract [5]. Another theory is the presence of tubular serous glands lining the tongue called Weber’s glands, which extend into the tonsillar fossa and above the capsule of the superior pole. The glands send a common duct to the tonsil and secrete saliva on to the surface of the tonsillar crypts. These glands are often left behind following tonsillectomy. After tonsillectomy, these glands may be a potential source for abscess formation. Therefore, attention should be given to excise any associated Weber’s gland or manage related branchial anomalies properly, when conducting tonsillectomy in cases with a history of quinsy. Other potential causes of PTA formation reported are dental disease, trauma, foreign bodies, tubercular granulomas and syphilitic gummata [6]. A parapharyngeal abscess should also be considered in the differential diagnosis of a peritonsillar abscess [7]. In 2.3% of cases with peritonsillar abscess, the abscess boundaries may extend to the parapharyngeal space. The case may appear clinically atypical, with inflammatory swelling of the pharyngeal wall below and behind the tonsil, edema of the epiglottis and a diffuse swelling on the side of the neck. The typical signs of peritonsillar abscess, i.e. trismus, a medially displaced tonsil and displacement of the uvula toward the opposite side, could be either completely lacking or less pronounced than usual [8]. The limited range of motion in our case was thought to be due to the parapharyngeal extention of PTA. It has also been reported that tonsillectomy leads to local immunological changes that predispose to local infection. The removal of tonsils and adenoid, as a part of the lymphoid tissues of the nasopharynx and oral cavity, may also result in increased susceptibility to retropharyngeal and parapharyngeal abscesses or phlegmons [9]. The abscess or phlegmon probably occurs as a result of an infection in the nasopharynx, sinuses or middle ear, which eventually spreads to lymph nodes of the retro- or parapharyngeal space. Affected lymph nodes are located between the posterior pharyngeal wall and the prevertebral fascia for retropharyngeal abscesses, or between the lateral pharyngeal wall and the superficial layer of the deep cervical fascia for parapharyngeal abscesses [9]. In pediatric patients a proper examination is sometimes harder, because of smaller oropharynx compared with adults, rather decreased level of cooperation, and presence of trismus. In these cases, the use of CT with contrast is reported to be sensitive in differentiating peritonsillar cellulitis from PTA and PTA from parapharyngeal involvement. CT also aids in following response to medical therapy, particularly non-complicated abscesses and in pediatric populations, or determining the route of drainage, if required [9,10]. However, there is a growing awareness of radiation exposure which prohibits this modality from being considered as the standard method of diagnosis in children, and in fact, a recent prospective study reports in the favor of transcervical ultrasonography (US) which proves it to be an excellent tool in the differentiation of PTA and cellulitis [11]. In our case, the abscess was demonstrated on CT examination as a homogenous hypodense abscess showing peripheral contrast involvement in the left parapharyngeal- peritonsiller space 2.7x1.6 cm in dimensions. The patient was started on IV antibiotic therapy rightaway and the trismus, palatal erythema and edema subsided without necessitating drainage or surgical intervention. The reported case was diagnosed with Kawasaki disease (KD) a year ago. He had symptoms of classic form, and recovered with IVIG therapy. KD is a pediatric illness characterized by prolonged high fever, mucocutaneous lesions and lymphadenopathy. It is potentially fatal as coronary arteritis occurs in up to a third of affected children. The presence of cervical adenopathy is considerably more frequent in the classic versus the atypical form of KD. If a febrile child presents with cervical adenitis, KD should be considered, as this may represent an early stage of the disease. Cases of cervical adenitis associated with other symptoms, such as exanthems, oral mucosal changes or conjunctivitis, should be evaluated for KD [12]. Additionally, KD may present with deep neck infections, such as a peritonsillar abscess, peritonsillar or deep neck cellulitis, suppurative parapharyngeal space infection, retropharyngeal cellulitis or mass [13,14]. There are two cases of KD reported in English literature presenting with peritonsillar abscess. Both of these cases presented with PTA and fever persisting despite appropriate IV antibiotics, incision and drainage, and even quincy tonsillectomy in one of the cases. The diagnosis of KD could only be made a week after admission, when finally further signs and symptoms of KD had developed. Both patients’ symptoms resolved with aspirin and IVIG. KD has a low recurrence rate, 6.89 per 1000 person-years, with a high incidence within the 12 months following the first episode. The incidence is reported to be high among those under 3 years of age and those with cardiac sequelae during the first episode [15]. Our case, had a KD history, and presented with PTA a year after the diagnosis of KD. In fact, he is the first case having PTA after tonsillectomy and history of KD. However, the abscess was not thought to be related to the prior KD history because the patient quickly responded to IV antibiotics, and none of the other symptoms of KD developed in the follow-up. PTA formation after tonsillectomy is extremely rare in the pediatric population. In this case report, we aimed to give an insight to the development of peritonsillar abscess after tonsillectomy. In the absence of remnant tonsil tissue, potential causes include infection of a second branchial cleft fistula, infection of Weber’s glands and dental disease. Tonsillectomy may also result in local immunological changes and may lead to an increased susceptibility to retropharyngeal and parapharyngeal abscesses or phlegmons. CT is has been reported to be a sensitive tool in pediatric cases as it helps in the differentiation of location of the abscess, enhancing diagnostic accuracy and obviating unnecessary drainage procedures, while transcervical USG is recently proven to be useful in providing these advantages without the risk of radiation. Successful treatment of PTA involves needle aspiration or incision and drainage and antibiotics. However especially pediatric cases may be treated conservatively without surgical drainage. KD may be predisposing factor for the formation of PTA. References
Presented atThis case report was presented in the 35th National Otorhinolaryngology and Head and Neck Surgery Congress as a poster in November 2-6th , 2013. |
|||
| Keywords : Tonsillektomi , peritonsiller abse , Kawasaki hastalığı , parafaringeal abse , derin boyun enfeksiyonu | |||
|