

Authors
|
|||||
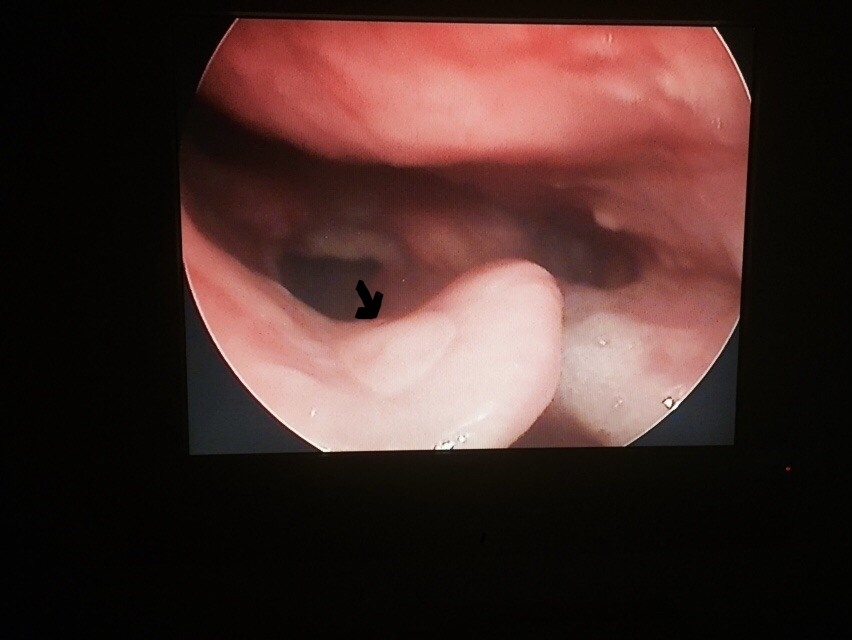
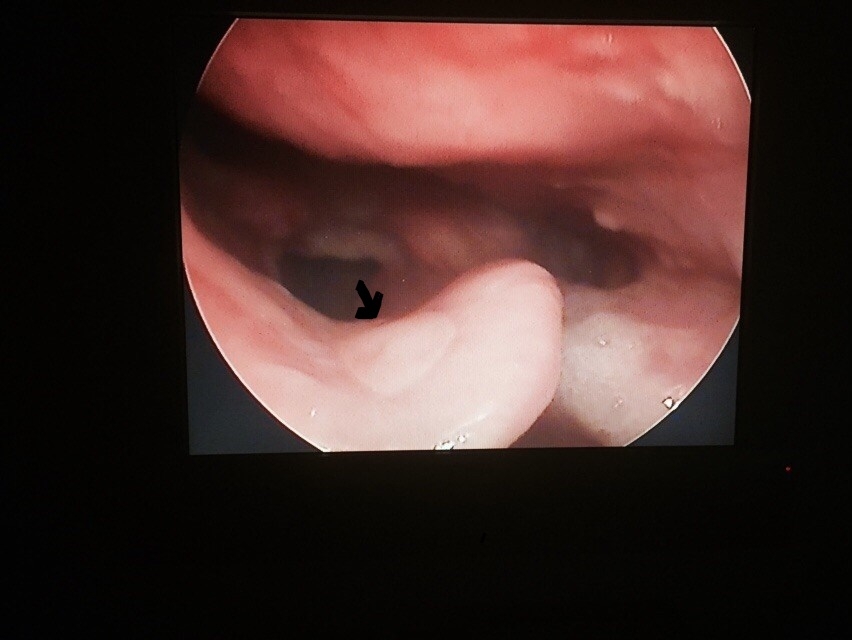
AbstractPemphigus vulgaris (PV) is a rare autoimmun disease characterized by clinically blistering of the skin and mucosa as a result of IgG antibodies against desmosomal proteins of squamous epithelia. 56-year-old male patient was referred to our clinic with the complaints of shortness of breath, hoarseness, dysphagia and throat pain for 3 months and the complaints were intensifying for the last 20 days. Erosive lesions were observed on laryngeal mucosa. Skin biopsy confirmed the diagnosis of pemphigus vulgaris. 1 mg/kg/day dose methylprednisolone was started and at Day 4, the patient’s complaints were subsided. At 7th day, endoscopic laryngeal examination showed completely healed lesions and significant decrease of edema.IntroductionPemphigus vulgaris (PV) is a rare autoimmun disease characterized by clinically blistering of the skin and mucosa as a result of IgG antibodies against desmosomal proteins of squamous epithelia [1]. The diagnosis of PV should be suspected in any patient with mucocutenous erosions or blisters. Mucosal regions are the first site of involvement in the majority of cases and PV may remain confined to the mucosal surfaces or extend to involve the skin. Oral mucosa is the most often involved area, larynx, pharynx, nasal mucosa may also be involved. Erosions, bullae,ulcer, crusting and aphthous-like lesions can be seen by endoscopic examination [2,3]. A skin or mucosal biopsy should be taken for histopathological and direct immunofluorescence (DIF) examination [1,2]. The characteristic findings consist of suprabasal acantholysis and intraepidermal blister formation. DIF demonstrates a chicken wire pattern of intercellular IgG in perilesional skin [2]. Autoantibodies in PV are most commonly directed against Desmoglein 3 [3-5]. The presence of antibodies to both Desmoglein 1 and Desmoglein 3 correlates with mucocutaneous disease [2-6]. We present a case of pemphigus vulgaris with laryngeal involvement. Case Report56-year-old male patient was referred to our clinic with the complaints of shortness of breath, hoarseness, dysphagia and throat pain for 3 months and the complaints were intensifying for the last 20 days. Before admitting to our clinic, the patient had diagnosis of acute pharyngitis in another center and prescribed amoxicillin-clavulanic acid for one week using 1 g 2x1, the patient’s complaints were increased after the treatment. The patient was admitted to a second center and diagnosed as laryngeal candidiasis then received oral nystatin. MR imaging was performed due to the increase of complaints and no obvious pathology in the oropharynx and larynx was reported. Indirect laryngoscopy revealed that there was widespread edema and bullous lesions around epiglottis, aryepiglottic folds and hypopharynx (Figure 1). There were no pathologic lymph nodes in the neck. Otoscopic and rhinoscopic examinations were normal.
Serology and bacterial culture test ruled out inflammatory and autoimmune diseases, viral and fungal infections and specific infections such as syphilis and diphtheria. There was an eroded lesion in the infero-lateral of the right knee which lasted for two weeks (Figure 2).
Pemphigus vulgaris was suspected during the dermatologic examination of the patient. Skin biopsy confirmed the diagnosis of pemphigus vulgaris. 1 mg / kg / day dose methylprednisolone was started and at day 4, the patient’s complaints were subsided. At 7th day, endoscopic laryngeal examination showed completely healed lesions and significant decrease of edema. Laryngeal mucosa was completely normal after 14 days. The skin lesions are topically treated with mometasone furoate and steroid therapy was terminated tapering on day 21. Erosive lesions in the nasal mucosa was observed during second month control endoscopic examination. Informed consent about steroid therapy was given by the patient. A year after initial therapy, there was no skin or laryngeal lesions. DiscussionPV is a life threatening autoimmune bullous disease, mediated by autoantibodies directed against antigens on the keratinocyte cell surface of stratified squamous epithelia [2]. Two clinical subtypes of PV defined:the mucosal form of PV and the mucocutanous form. The frequency of ear nose and throat involvement in PV is not clearly defined [7]. Mucosal lesions were seen in 90% of PV patients, however, 46% of them are not accompanied with skin lesions. The most common ENT symptoms are sore throat (56%) and hoarseness (39%) in PV patients. All identified mucosal lesions are superficial and mild hyperemia [6]. Oral symptoms and oral active PV lesions were the most frequent findings (94%). Laryngeal lesions were most commonly present in mucosal form [7]. Laryngeal involvement in pemphigus or pemphigoid may vary in severity from a light hoarseness to a serious oedema leading in airway obstruction and emergency tracheostomy. However, the common findings are: oedema, ulcerations, bullae, membranes, and stenosis. Intubation is usually not recommended in order to avoid injuries in a fragile larynx [8]. According to Ohki et al, the most frequent sites of membrane lesions included the gingiva, buccal muccsa, soft palate, epiglottis, vocal fold, and nasal septum [9]. Aizawa et al. reported that nose is suspectable to developing pemphigus lesions [10]. PV must be approached in a multidisciplinary fashion cause mucosal disease is a type of skin involvement may occur without the involvement of pemphigus and should be remembered that the other isolated laryngeal lesions and skin and mucosal lesions may occur later. Long-term hoarseness and sore throat which is not improving with medical therapy, PV should be considered as a possible diagnosis. References
|
|||||
| Keywords : Larinks , Pemfigus vulgaris , boğaz ağrısı | |||||

|