

Authors
|
|||||||
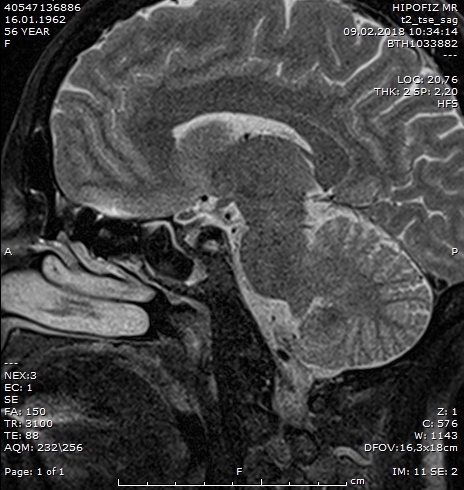
AbstractWe report a rare case of isolated sphenoid ‘fungus ball’ presenting as vision loss and headache. Sphenoid fungus ball also called as mycetoma is a rare disease and it causes nonspecific symptoms such as headache, visual disturbance and cranial nerve palsies. Diagnosis usually made after imaging studies for non-specific symptoms. In this report, we present a case of isolated sphenoid fungus ball with the symptoms of vision loss and severe headache. Symptoms subsided after sphenoidotomy and clearance of fungus ball.IntroductionSphenoid sinus mycetoma or ‘fungal ball’ associated vision loss is a rare condition and there are only four reported cases of sphenoid fungal ball in conjunction with vision loss and severe headache [1]. Symptoms and treatment strategies are the same as isolated bacterial infection of sphenoid sinus which is also a rare disease. The most commonly encountered isolated sphenoid sinus lesions (ISSD) are sinusitis, fungal infection, mucoceles, or tumors and fungal infections are the third most common cause of ISSD lesions (14.5%) [1]. Patients usually have asymptomatic during the early stages of the disease, symptoms appear when inflammation becomes more serious. Isolated sphenoid sinusitis caused by fungus is much rarer, and is more difficult to detect due to the nonspecific symptoms and absence of any characteristic signs during endoscopic examination [2-8]. Recently, the detection rate of ISSD has increased because of the development of imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI). Aspergillus fumigatus is the most common causative fungus isolated from sphenoid sinus, as well as from the paranasal sinuses. Important structures such as cranial nerves, carotid artery and cavernous sinus are related closely to sphenoid sinus. We report a case of isolated sphenoid fungus ball presenting with severe headache and vision loss. Case Report56 year old female patient admitted to our clinic with the symptoms of severe headache and vision loss. The patient has admitted to different neurology and neurosurgery clinics for the complaints of headache and vision loss. MRI examination revealed a mass in the left sphenoid sinus and the patient was referred to our clinic. ENT examination was normal. Ophtalmologic examination revealed that the patient’s vision was limited to light perception. MRI examination revealed a mass filling left sphenoid sinus. The mass has isointense nodularity with the mucosa on the coronal precontrast T1-weighted image (Figure 1) and a low signal on the T2-weighted sagittal image (Figure 2). The sinus mucosa has enhancement was shown on axial gadolinium enhanced T2-weighted image (Figure 2). Restricted diffusion was not observed.
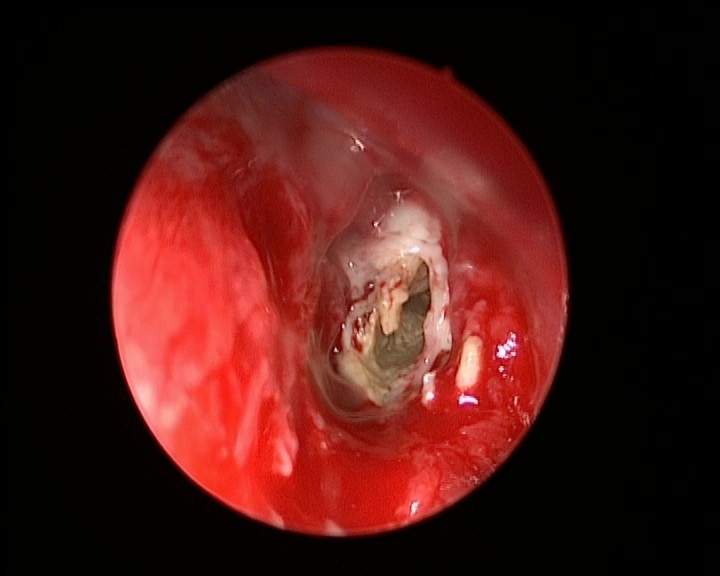
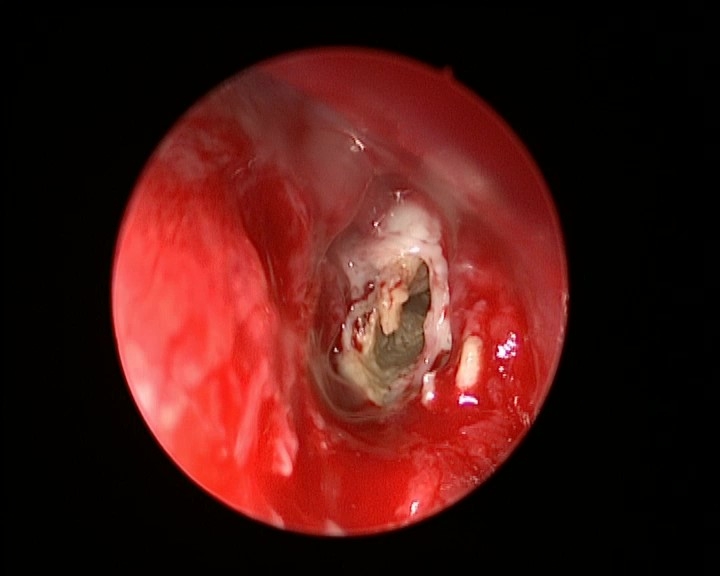
The surgery was performed under general anaesthesia. Pledgets moistened with epinephrine were packed into the nasal cavity (between the nasal septum and the middle turbinate) for vasoconstriction, after which 2% lidocaine with 1:100,000 epinephrine was used for the local infiltration under 0° scope. When sphenoidotomy was performed through the paraseptal approach, the superior turbinate was identified first and was partially resected to widen the sphenoethmoidal recess. After the identification of the sphenoid ostium, using Lucae forceps or a suction tip, we enlarged the natural ostium of the sphenoid to complete the sphenoidotomy. Fungus ball was observed and removed gently using suction and freer elevator (Figure 3). Finally, sinus irrigation with normal saline solution was performed to completely remove any fungal debris from the sphenoid sinus.
The symptoms were completely recovered after the surgery. Follow up of the patient was performed on weekly basis by endoscopic examination. Crusts and discharge were removed during the first postoperative month. We recommended the patient to perform nasal irrigation with saline solution 3 times a day for at least 1 month. DiscussionThe incidence of isolated fungal sphenoid sinusitis is very low. Most cases of isolated sphenoid fungal disease are characterised by a fungal ball, accounted for 31 percent of inflammatory sphenoid disease incidence [5]. However, Lawson et al. found that the incidence is only 7.5 per cent [4]. Sphenoid fungal sinusitis is difficult to diagnose in its early stages, due to the inaccessible position of the sphenoid sinus and the unremarkable inflammatory presentation with nonspecific symptoms. Fungus ball is most commonly seen in the maxillary sinus (82.7% – 94.0%), followed by the sphenoid sinus (4.0% – 14.4%) [8]. Headache is the most common symptom [9]. The most common region of headaches in isolated sphenoid fungus ball was found to be nonspecific [8,9]. In the literature, visual disturbance is reported to be a common symptom, with incidence ranging from 14% to 52% in ISSD and isolated sphenoid fungus ball [9,10]. The possible reasons for visual problems are cranial neuritis, pressure ischemia, and ischemic infarction. Grillone et al. showed that the optic nerve is affected by sphenoid sinus fungal balls more often than any other cranial nerve [11]. Lee et al. reported that the %54 the optic nerve (54 percent) followed by the abducens nerve (40%) [8]. The optic nerve involvement is probably due to the local anatomy of the region. In a study, it is found out that 79% of cadavers, the inner wall of the optic canal is less than 5 mm thick, and it is completely absent in 8% [8]. Bowman et al. advised the use of CT scanning as the primary imaging tool and have described the characteristic findings of the sphenoid fungus ball including intralesional calcification (100%), sclerosis of sinus wall (82%), total sinus opacification (82%), enlarged sinus (76%), and sinus wall erosion (52%) [10]. MRI is superior for demonstrating the interface with surrounding cranial structures and vascularity of the lesions, therefore, it is important to rule out vascular lesions by using MRI. Endonasal endoscopic sphenoidotomy is regarded as a primary therapy in the treatment of an isolated sphenoid sinus fungal ball [9,10]. Bowman et al. reported complete resolution in all of the cases underwent this procedure [10]. In conclusion, isolated sphenoid fungus ball is a rare disease with non-specific symptoms and signs. Fungus ball mostly seen in older women and the proper diagnosis of this disorder requires the appropriate application of radiologic imaging including CT and MRI. We believe that early diagnosis and proper intervention is essential in patients to prevent serious complications such as vision loss. References
|
|||||||
| Keywords : Sfenoid sinüs , mantar , baş ağrısı , görme kaybı | |||||||

|