

|
|||
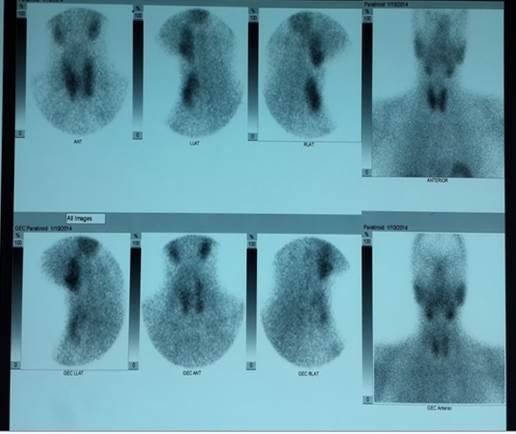
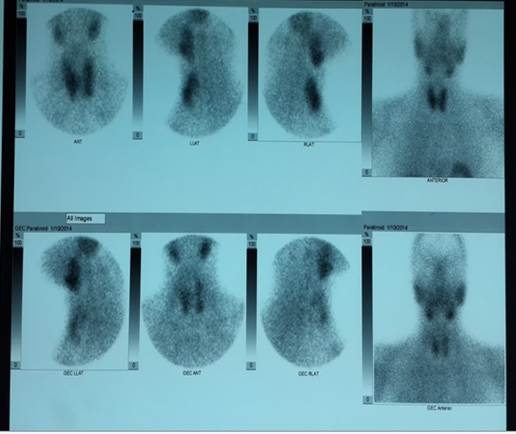
AbstractSecondary hyperparathyroidism is a serious common complication caused of prolonged dialysis. Tertiary hyperparathyroidism occurs in patients with a history of chronic renal failure after successful renal transplant. Secondary and tertiary hyperthyroidism are always associated with hyperplasia involving multiple parathyroid glands. We present a case report of a patient who was undergoing total thyroidectomy and subtotal parathyroidectomy for tertiary hyperparathyroidismand thyroid nodules, but was found to have “- quadruple gland parathyroid adenoma” based on pathology results after enlargement of all parathyroids were observed. To the best of our knowledge, this finding has not been reported in the literature before now in a patient with tertiary hyperparathyroidism.IntroductionSecondary hyperparathyroidism (SHPT) is a common serious complication caused by prolonged dialysis. SHPT begins with the reduction of renal function and is promoted by impaired excretion of phosphorus, calcitriol deficiency and hypocalcaemia [1]. Tertiary hyperparathyroidism (THPT) occurs in patients with chronic renal failure following successful renal transplant. It is believed to result from a gradual loss of parathyroid function over time in response to changes in serum calcium and phosphate. Although THPT is not common in renal transplant patients (1.6% – 3% in some series),[2-5] it may cause serious complications (e.g., pathological fractures, joint disease, urinary calculi, mental status changes, muscle weakness, peptic ulcer disease, and pancreatitis) [5,6]. Surgery remains the only curative treatment of THPT [2,4]. Subtotal or total parathyroidectomy with autotransplantation is the standard surgical approach to patients with THPT. To the best of our knowledge, quadruple-gland parathyroid adenoma in THPT has not yet been reported in the literature. Case ReportA 45 year old woman with a past medical history of renal transplant two years ago, hypertension, peptic ulcer disease and nephrolithiasis was referred to us by her endocrinologist due to multi-nodular goiter and hypercalcemia. On physical examination, she was noted to have a diffusely palpable thyroid. Serum chemistries showed a markedly elevated serum calcium (11.8 mg/dL) and PTH (1129 pg/mL): vitamin D level was 8 ng/mL; phosphorus, 2.9 mg/dL and creatinine, 0.56 mg/Dl. Dual-energy X-ray absorptiometry demonstrated osteoporosis (spine T-score, −3.28; hip T-score, −2.70). Thallium-201 and 99mTc pertechnetate thyroid scans were within normal limits (4.8 × 2.4 cm, right lobe; 4.2 × 2.7 cm, left lobe). Delayed static images of the neck after 99mTc-sestamibi injection showed abnormal tracer accumulation in areas in the superior and the inferior left thyroid lobe, suggestive of adenoma or hyperplasia. There was no significant difference compared to a scintigraphy study performed two years prior. (Figure 1) Ultrasound of the thyroid gland showed a normal-sized gland (left lobe, 4.2 × 1.8 × 1.8 cm; right lobe, 4.1 × 2.6 × 1.4 cm). However, we observed multiple thyroid nodules with different characteristics within the thyroid, including a 14 × 7 mm (the largest) heterogeneous hypoechoic nodule and an 11 x 10 mm cystic hypoechoic nodule in the lower zone of the right lower lobe. Ultrasound-guided fine needle aspiration biopsy of the thyroid nodules in the right lobe showed benign follicular cells.
An interdisciplinary council adjudicated that continued medical treatment of patient’s hypercalcemia would be ineffective; therefore, it was decided to proceed with total thyroidectomy and subtotal parathyroidectomy. After total thyroidectomy, however, all quadruple parathyroid glands were found to be enlarged, and total parathyroidectomy with autotransplantation of approximately one-half of a gland into the sternocleidomastoid muscle was performed instead. The patient was followed up for four years after the operation. The patient did not have signs of disease recurrence or hypocalcaemia. DiscussionTHPT is caused by excessive secretion of PTH as a result of a prolonged SHPT and the development of hypercalcemia. These two hyperparathyroid states are also called “renal hyperparathyroidism”. Over the last 50 years, surgeons have debated the most appropriate surgical approach for parathyroidectomy in renal transplant patients because each has advantages and disadvantages. Subtotal parathyroidectomy, first reported by Stanbury in 1958, is still the most frequently surgical method used to date [7]. This surgical approach is based upon the theory that all quadruple[or more] glands undergo hyperplasia with THPT [5,7], and the fact that it is now generally agreed upon that double adenomas represent a separate clinical entity [8-10]. The surgical choice in patients with SHPT depends on the preference of the surgeon [11] . Initially, we planned to do a subtotal parathyroidectomy, but we made the decision to perform total parathyroidectomy with autotransplantation after finding that all of the parathyroid glands were enlarged. Some authors advocate this surgical technique due to convenience in the case of. parathyromatosis by studying in a very limited area by protecting the blood supply and a little of the the gland capsule [12] . We are also aware of these in subtotal parathyroidectomy surgery, but] We did not an attempt to preserve any parathyroid tissue in its native location because the patient required total thyroidectomy for bilateral thyroid nodules. When followed post-operatively, our patient did not have hypocalcaemia, or “hungry bones syndrome”. Pathology results from her thyroid gland showed papillary carcinoma, follicular variant. Although the the occurrence of recurrent hyperparathyroidism and differentiated thyroid cancer together is very rare, there is evidence to suggest that chronic renal failure may be a predisposing factor for malignancy. If so, this patient may represent a case representing this association. Lai reported that renal hyperparathyroidism is always caused by parathyroid hyperplasia in multiple glands [13] . Although diffuse hyperplasia of the parathyroids is expected in specimens from patients with chronic renal failure undergoing parathroidectomy, this is the first report of quadruple-gland adenoma with THPT of which we are aware.
References
|
|||
| Keywords : Tersiyer hiperparatiroidizm , dört adenom | |||
|