

Authors
|
|||||||||||||
AbstractSchwannomas are benign tumors originating from Schwann cells that form the myelin sheaths of axons in peripheral nerves. These tumors may appear in various body parts, with 25% of them found in the head and neck region [1]. Schwannomas of the middle ear may originate from the facial nerve, tympanic chord, tympanic branch of the glossopharyngeal nerve (Jacobson nerve) or auricular branch of the vagal nerve (Arnold nerve).IntroductionSchwannomas are benign tumors originating from Schwann cells that form the myelin sheaths of axons in peripheral nerves. These tumors may appear in various body parts, with 25% of them found in the head and neck region [1]. Schwannomas of the middle ear may originate from the facial nerve, tympanic chord, tympanic branch of the glossopharyngeal nerve (Jacobson nerve) or auricular branch of the vagal nerve (Arnold nerve). Case ReportAn 17-year-old male patient presented with a plugging sensation in his right ear for 4 months. His complaint began after diving into the sea. He had no history of vertigo, tinnitus or otorrhea. Upon the physical examination of the patient, the right tympanic membrane was intact but cambered, and there was a soft tissue image behind the malleus. The audiometric test revealed to the patient. The result for left ear was normal and there was conductive hearing loss in the right ear. His facial nerve functions were intact. He had no sign of neurofibromatosis. Upon magnetic resonance imaging of the inner ear, an 11x9 mm mass with massive contrast uptake and intermediate intensity after intravenous contrast (IVC) was observed on the T1 and T2-weighted sequences and in the nodular configuration at the level of the mesotympanum and epitympanum.
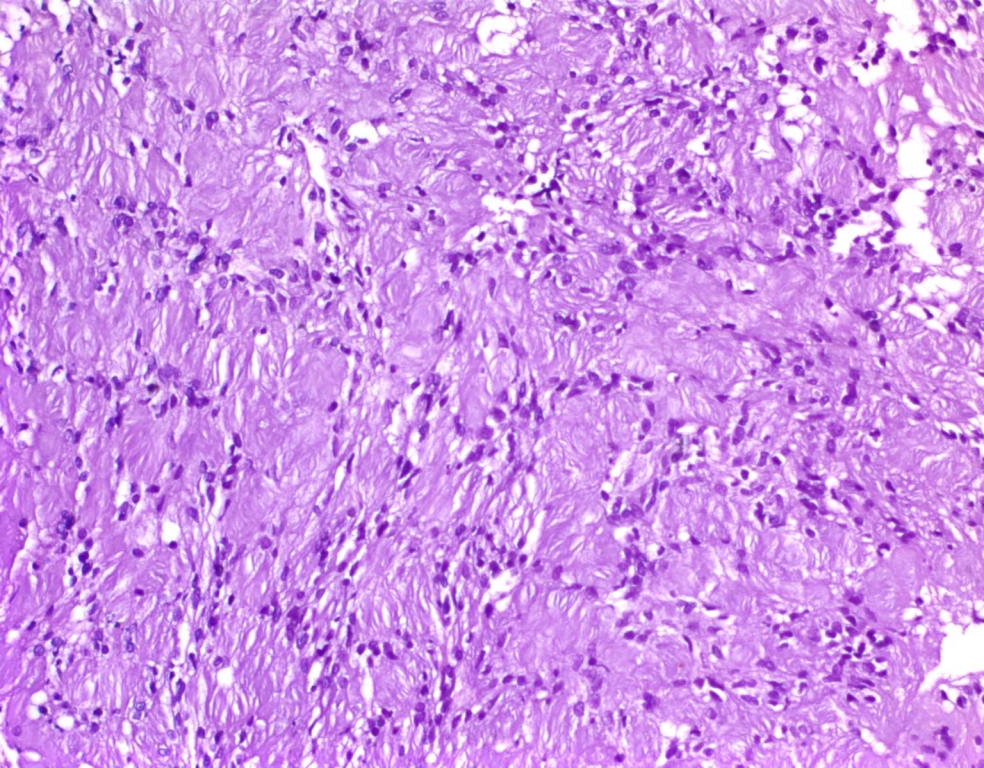
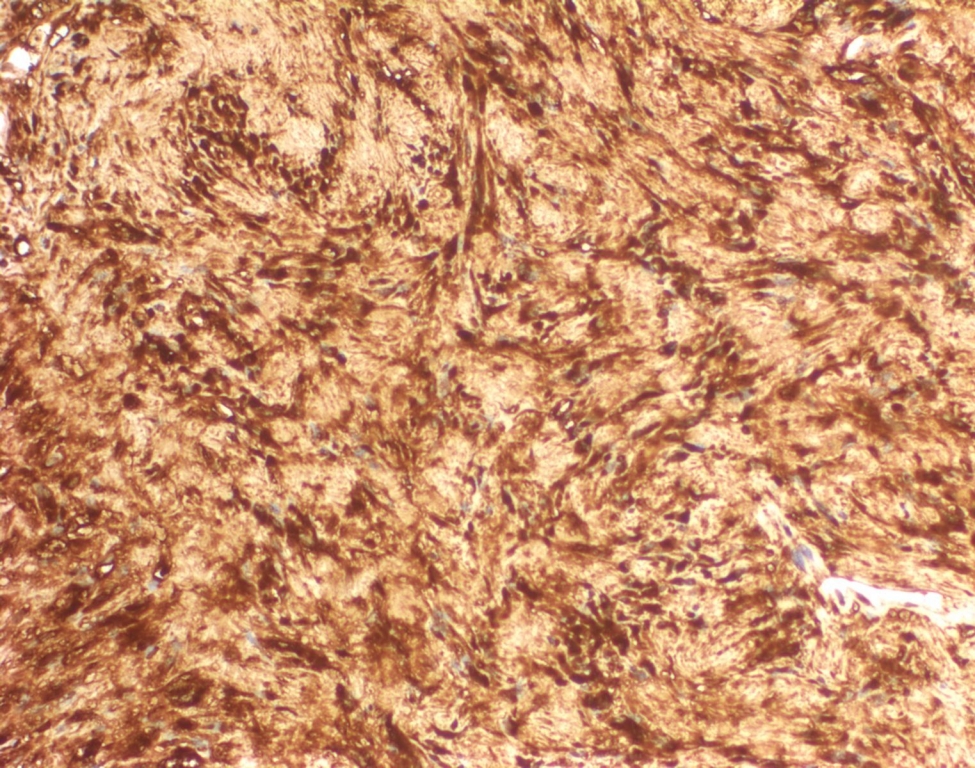
The patient underwent explorative tympanotomy with a postauricular approach. The mastoid cells were exposed by opening the mastoid cortex. The antrum was clean. There were pale-colored tissues on the promontorium in the middle ear extending to the epitympanum. These were partially removed with cup forceps and sent for freezing. The results of the freezing indicated polypoid tissue containing collagenized connective tissue stroma. The entire tissue was removed, and the facial channel was intact. A graft was prepared using the temporal muscle fascia and was spread over the malleus from the posterior wall of the external auditory canal towards the anterior. The pathological diagnosis of the mass indicated a schwannoma. The postoperative functions of the facial nerve were intact. Postoperative audiology tests revealed that the gap in the right ear was closed, and the hearing thresholds became normal. Histologically, the tumor was composed of spindle cells that were arranged in a palisading fashion.
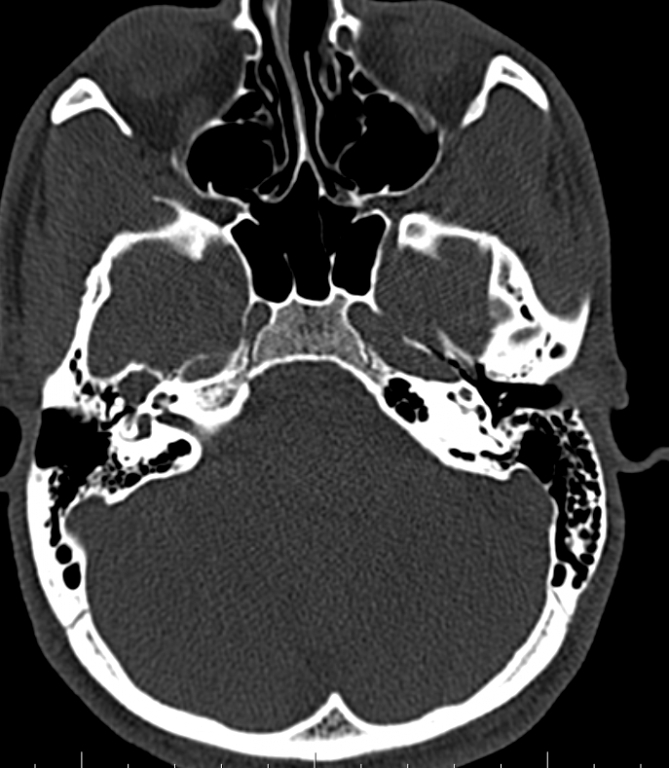
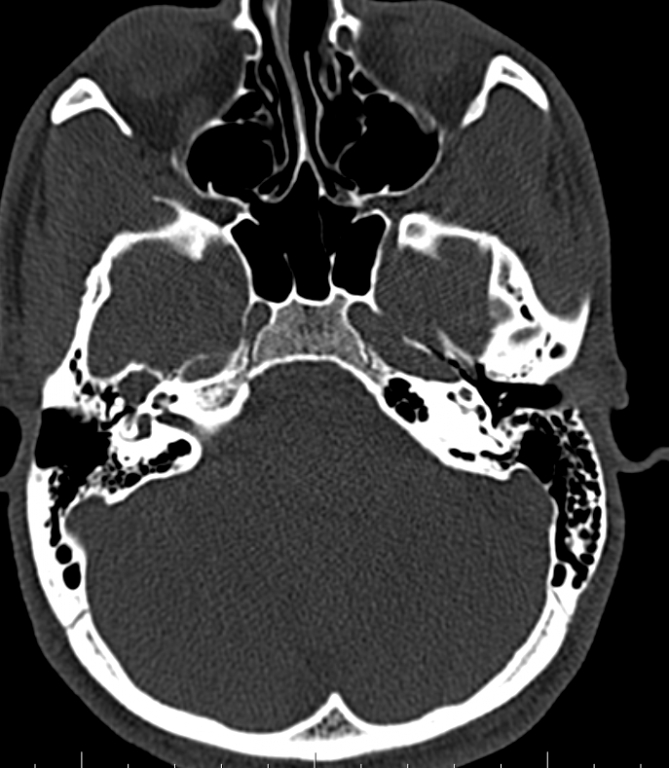
One year later he came to control a year after the surgery. Upon CT of temporal bone, tumor regrowth was observed at epitympanum again which looked like the schwannoma recurrence.
DiscussionSchwannomas of the middle ear originate from facial nerves, tympanic chords, tympanic branches of the glossopharyngeal nerve or the auricular branch of the vagal nerve [1]. The facial nerve is the most frequently involved nerve in middle ear schwannomas [2,3]. Facial nerve schwannomas may cause facial paralysis and conductive hearing loss. It has been reported that, in some cases, the mass was incidentally detected during middle ear surgery, even though no facial paralysis was found [4]. Moreover, facial nerve schwannomas may originate from any segment of the facial nerve, and mostly originate from the tympanic segment. In cases where schwannoma is suspected, the approach should be similar to that for facial nerve schwannoma, and a biopsy must be avoided in order not to cause facial paralysis [1]. A dilemma for deciding whether to perform surgery arises when a facial nerve schwannoma is suspected in patients with intact facial nerve functions. However, it is impossible to make a definite diagnosis with exploration without performing a biopsy. Schwannomas originating from the tympanic chord have also been reported. Such patients typically have hearing loss and normal facial nerve functions. The lesion otoscopically appears as a convexity in the posterosuperior aspect of the tympanic membrane or on the posterior wall of external auditory channel. As is also observed in the present case, an otoscopic examination can reveal a convexity in the tympanic membrane. These convexities can be determined in the early phase of growth and can be removed without causing facial nerve injury. The Jacobson nerve, which is responsible for the sensorial innervation of the parotid gland, is the first branch of the glossopharyngeal nerve and is formed after passing the jugular foramen. It provides sensorial branches to the mesotympanum and Eustachian tube and joins with the caroticotympanic nerve to form the lesser superficial Petrosal nerve. Promontorium erosion, together with an intact facial channel, is a significant indicator that the tumor is derived from the Jacobson nerve [5]. MRI revealed isointense and homogenous contrasting in the brain on T1 and T2 sequences. In the present study, the MRI of the internal acoustic channel demonstrated a mass with massive contrast uptake and intermediate intensity after IVCA on T1- and T2-weighted sequences. The Inner ear CT demonstrated a lesion without contrast at the right attic level extending to the mesotympanum that slightly eroded the surrounding bone tissue without causing impairment in the integrity of the middle ear ossicles. During surgery, it was observed that the facial channel was intact, and the mass was tightly attached to the promontorium when it eroded the promontorium. Based on these radiological, clinical and intraoperative findings, firstly we thought that the mass to be a Jacobson nerve schwannoma, but postoperatively the mass occurred at epitympanum again so we considered the mass to be a facial nerve schwannoma. About treatment we can follow up this schwannomas or we can operate his mass. Also the mass can be treated with gama knife. But gama knife is not a good alternative for a limited schwannoma in the middle ear. Conclusion Middle ear schwannomas are rare; among these, Jacobson nerve schwannomas are even more rare and are very difficult to diagnose. It is necessary to differentiate these tumors from facial nerve schwannomas and from overall middle ear schwannomas. Jacobson schwannomas may erode the promontorium, but this is not pathognomonic. When facial nerve schwannoma is suspected, no biopsy should be performed to avoid facial nerve paralysis. However, exploration must be completed in cases in which bone destruction occurred due to the tumor and according to apparent clinical symptoms. References
|
|||||||||||||
| Keywords : schwannoma , vertigo , schwann hücresi , periferik sinir | |||||||||||||



|