

|
|||
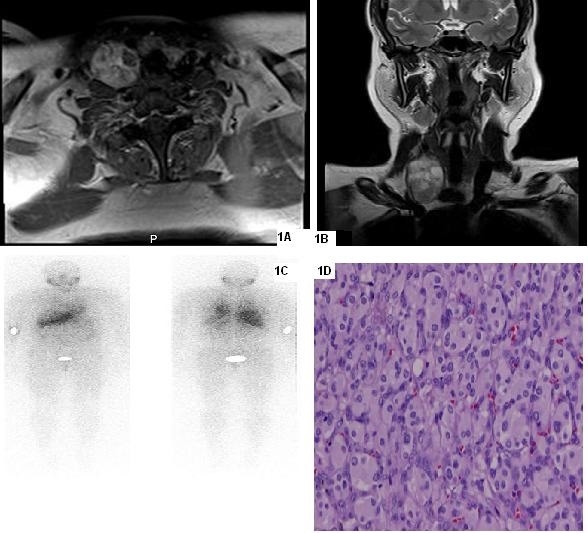
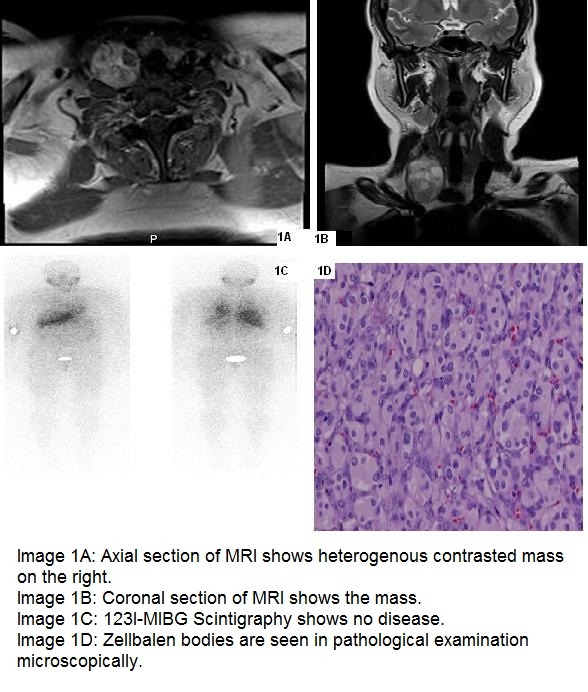
AbstractParagangliomas are neuroendocrine tumors which develop from extra-adrenal paraganglia tissues. This tissues derivate from neural crest and relate to autonomous nerve system. Head and neck paragangliomas are generally non-functioned unlike pheochromocytoma. The first symptom is slow-growing mass in neck usually. A 42-year-old woman was admitted to otolaryngology clinic with the complaint of neck mass which was slow-growing. There was a 5 cm, painless, semi-mobile mass in her right neck. There was no other pathological finding. It was a 33 mm mass behind the carotis in ultrasound examiation. It was hypervascular and including cystic areas. There was a 5 cm tumor which developed from the right vagal nerve in the operation. Vagal nerve was sacrified to remove tumor. Specimen was consistent with paraganglioma. An unusual infrahyoid vagal paraganglioma case was presented in this paper. There is only one report about such a disease before in English literature.IntroductionParaganglioma (PG) is a neuroendocrin tumor which develops extra-adrenal paraganglia cells. It is related to sympathetic or parasymphatetic system. Head and neck PG (HNPG) usually develops parasymphatetic system. PG is called according to its developed area; carotid, jugular, tympanic or vagal. Chemodectoma and glomus terms were used before, but paraganglioma is preferred now [1]. 1-3 % of HNPG secrete catecolamins [2]. They usually have multipl endocrine neoplasia (MEN) syndrome. 40 % of familial form and 10 % of sporadic form could be multipl [3]. The most common symptom of HNPG is painless, slow-growing mass in neck. HNPG is more common in women unlike other PGs [1]. 60 % of HNPG is related to carotid body. HNPG which develops from vagal nerve is under 5 %. [4]. Vagal PG is largely close to skull base and cranial nerves are effected more [5]. Although vagal PG could develop from everywhere of vagus nerve theoritically, it develops from ganglion nodosum generally [6]. A 42-year old woman who had infrahyoid vagal PG is presented in this paper. Case ReportA 42-year old women was admitted to clinic with the complaint of slow-growing neck lump. She had the lump for 6 years. She denied smoking or alcohol abuse, B symptoms and flushing attacks, contact of cats or rodents. She had no chronical disease. There was a 5 cm, semi-mobil, painless neck mass in the right supraclaviculer area in her physical examination. Vocal cord movements were normal bilaterally. There was no pathologic finding in the other examination. There was a 33x29 mm hypervascular hypoecoic mass in the right neck with cystic areas inferiorly and medially in her ultrasound (US) examination. The mass was behind the carotid arter and jugular vein. Fine needle aspiration biopsy (FNAB) could not be done because of its hypervascularity feature. There was no pathological condition about thyroid and lymph nodes. There was a 35x31x53 mm, heterogenous contrasted mass in magnetic resonance imagination (MRI) (Images 1A-1B). A neck exploration, excision and frozen section were planned for the treatment of patient. A mass which developes from vagal nerve was seen during operation. It could not be disected from vagal nerve. Therefore, vagal nerve was sacrified. She had hoarseness postoperatively, but she could swallow without aspiration. Her voice was normal after 6th month of surgery. 123-I metaiodobenzylguanidine scintigraphy (123I-MIBG) was done because of possibility of multipl disease and no disease was seen (Image 1C). Biopsy result was paraganglioma (Image 1D). There was no recurrens in a 2-year period.
DiscussionPG is 0.6 % of head and neck tumors [7]. HNPG is usually related to parasymphatetic system and does not secrete cathecolamins [1]. Vagal PG is common in middle-aged women. Patients exhibit slow-growing neck mass largely. When PG causes cranial nerve paralysis, they can be admitted with cranial neuropathy symptoms. Although it is usually negative, urinary cathecolamin examination must be done because of possibility of associated pheochromacytoma or other PG [8]. Urinary cathecolamin test was not done in the patient because of its unusual location. Computed tomography (CT) and MRI angiography are useful in the diagnosis. Vagal PG pushes forward external and internal carotid arteries. They are highly contrasted tumors. 123I-MIBG scintigraphy can be done for multipl disease [9]. Because of its atypical location and heterogenous contrasted view, PG was not thought in pre-diagnosis. Treatment of vagal PG is surgical. Vagal nerve is sacrified in almost case [10]. Although some examiners offer vocal cord medialization in the same seans, it is not accepted generally. If there is 10th and 12th nerve paralysis, aspiration risk is more [6]. There are some reports about preoperative embolization is useful for intraoperative bleeding [10]. Although vagal PG could develop from everywhere of vagus nerve theoritically, it develops from ganglion nodosum generally [6]. Infrahyoid vagal PG is very rare and there is only one case about it in the English literature. Saito et al. reported a infrahyoid vagal PG which was seen cathecolamin crisis during operation [11]. A very rare case, infrahyoid vagal PG, is presented in the paper. Sharing such this case enriches the literature and increases awareness. Vagal paraganglioma must be considered in pre-diagnosis especially in the patients have highly contrasted tumor behind the carotid artery. References
Presented atThe Turkish National Otolarungology - Head and Neck Congress, 2015 Antalya - Turkey |
|||
| Keywords : vagus , nöral krest , hyoid | |||
|