

Authors
|
|||
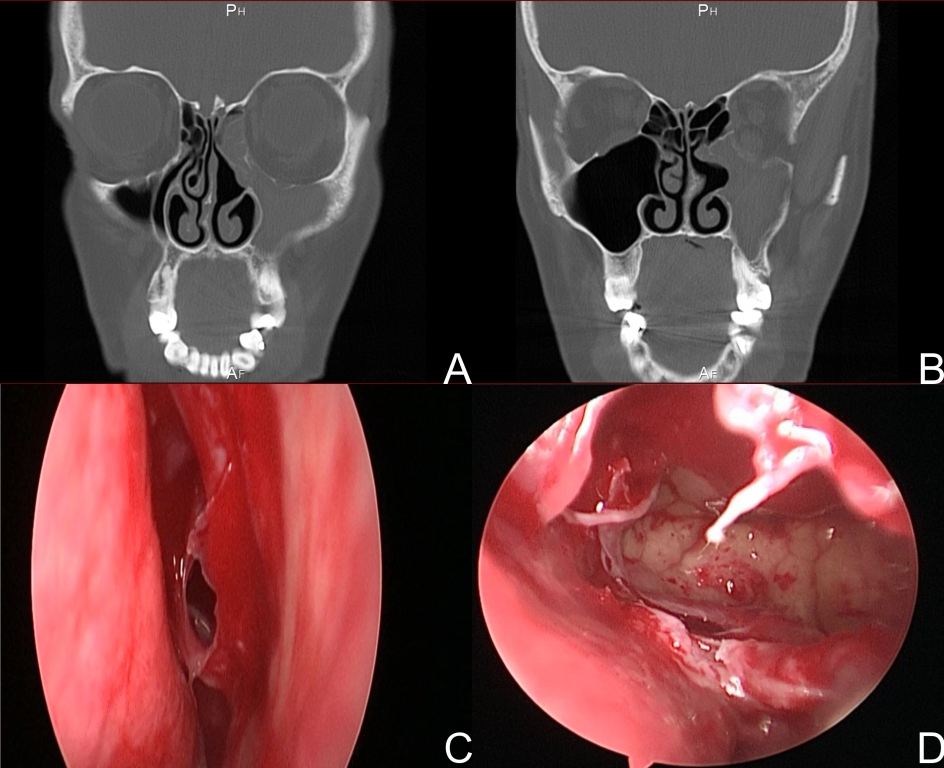
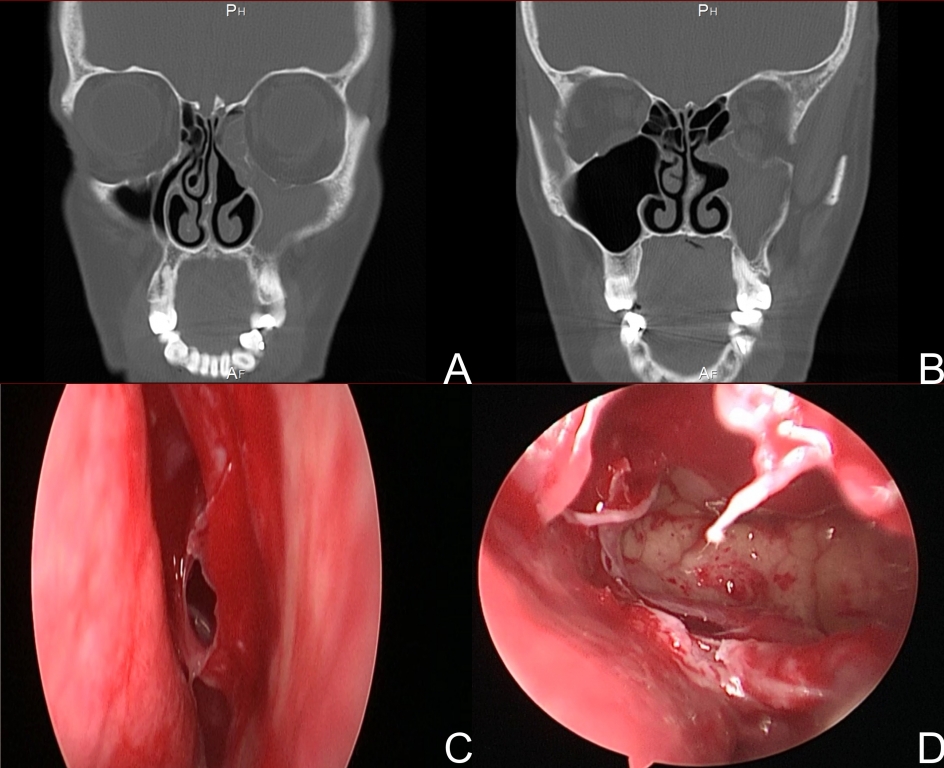
AbstractSilent sinus syndrome is a rare disease that causes painless enophthalmos and hypoglobus and is difficult to diagnose. A 61-yearold female presented at our clinic with the complaint of enophthalmos and hypoglobus of the left eye and facial asymmetry on the left half of the face. According to the clinical symptoms and imaging studies, silent sinus syndrome was suspected. Therefore, endoscopic surgery was applied to the patient. This uncommon case of silent sinus syndrome is presented in this paper.IntroductionSilent sinus syndrome (SSS), which was first described by Montgomery in 1964 and named by Soporkar in 1994, is characterized by enophthalmos and hypoglobus associated with an atelectatic maxillary sinus with ipsilateral sinus opacification [1, 2]. The main pathophysiology of SSS is still unknown, but it has been reported that sinus atelectasis of a unilateral maxillary sinus may cause osteomeatal occlusion, which may then lead to negative pressure and orbital floor depression [3, 4]. In the management of SSS, endoscopic maxillary antrostomy with or without orbital floor reconstructioncan be used. In this paper, a rare case of silent sinus syndrome is reported and the management options of this condition are discussed.Case ReportA 61-yearold female presented at our clinic with the complaint of enophthalmos and depression of the left eye and facial asymmetry on the left half of the face. Endoscopic nasal examination of the patient revealed over-lateralization of the middle turbinate in very close proximity to the lateral nasal wall. A computed tomography (CT) scan for paranasal sinuses was performed. The CT scan showed atelectasis and soft tissue enhancement in the left maxillary sinus and orbital floor depression (Figure1A-1B).The ophthalmic examination of the patient revealed enophthalmus and hypoglobus in the left eye, but the visual field examination results were normal. Silent sinus syndrome was suspected and endoscopic surgery was applied to the patient. Left maxillary antrostomy and middle turbinate medialization were performed and re-aeration of the left maxillary sinus was ensured (Figure 1C-1D). Orbital floor reconstruction was not necessary and follow-up was preferred. The patient was discharged from the hospital on postoperative day 2. At 12 months after the treatment, the patient is well without evidence of recurrence.
DiscussionSilent sinus syndrome is a rare disease that causes painless enophthalmos and hypoglobus and is difficult to diagnose. Patients present with facial asymmetry and hypoglobus as a result of spontaneous painless enophthalmos. The main reason for this condition is asymptomatic occlusive chronic mucosal sinus disease and hypoventilation caused by maxillary sinus hypoplasia [5]. The disease was first described by Montgomery in 1964 and then named 'silent sinus syndrome' in 1994 by Soporkar [1, 2].This syndrome occurs mainly in the fourth and fifth decades of life and is seen equally in both genders. However, there have also been reported cases in the pediatric population [6, 7]. Several conditions can mimic silent sinus syndrome, such as facial trauma, malignancies, and congenital defects, but the classical diagnosis of SSS requires spontaneous initiation and progression of the disease [7]. For a diagnosis of SSS, physical examination combined with radiological evaluation is of crucial importance. On physical examination, upper eyelid retraction, ptosis, dry eye, lagophthalmos, depression of the malar region, facial asymmetry and diplopia can be seen. Septum deformity, lateralized middle concha and uncinate process, and enlarged middle meatus may be seen in the endoscopic examination of the nasal cavity [8]. The main radiological technique for evaluation of paranasal sinuses is computed tomography (CT). Radiographic findings, such as uncinate process lateralization, inferomedial displacement of the orbital floor, and opacification of the ipsilateral maxillary sinus can suggest SSS [9]. Eyigör et al. evaluated atelectatic sinuses by using CT comparison with the healthy side in 16 patients. It was concluded that for patients with suspected silent sinus syndrome, maxillary sinus volume, retroantral fat mass, infraorbital bone angle, and uncinate process lateralization measurements could be used as objective tests [10]. The goal of SSS treatment is mainly to provide maxillary sinus ventilation and drainage and correct orbital anatomy. The Caldwell-Luc operation and functional endoscopic sinus surgery are the methods used in the treatment. In a Caldwell-Luc operation, first a gingivobuccal sulcus incision is made on the side of the pathologyand then the anterior maxillary wall is removed and inserted into the sinus. The ostium is expanded to provide drainage. In endoscopic surgery, first any septum deviation is corrected, then uncinectomy can be performed to reach the maxillary drainage system or the osteomeatal complex. After the uncinectomy, the maxillary sinus ostium is often seen and enlarged[11]. The timing of orbital floor reconstruction to resolve hypoglobus and enophthalmos is controversial. Some authors have argued that sinus surgery alone is sufficient, while others have recommended reconstruction after 2-6 months. Silicone blocks, teflon, bone graft, hyaluronic acid and cartilage may be used in the reconstruction of the orbital floor. Kashima et al. used nasal septal cartilage, ear cartilage, or LactSorb in 11 patients and reported that cartilage is very useful in stabilizing the orbital floor[12]. The treatment modality selected for the current patientwas the endoscopic approach to provide re-ventilation of the maxillary sinus, with follow-up for orbital floor reconstruction. After a 6-month follow-up period, the hypoglobus and enophthalmos symptoms were seen to have resolved spontaneously. Therefore, it should be emphasized that orbital floor reconstruction can be delayed until spontaneous resolution occurs. Conclusion Silent sinus syndrome, as seen in the case presented here, is a very important entity in clinical practice, of which practitioners should be aware. In the treatment of SSS, surgery should be the preferred method but orbital reconstruction may be delayed because of the high probability of the spontaneous resolution of symptoms. References
|
|||
| Keywords : Sessiz sinüs sendromu , maksiller sinüs atelektazisi , enoftalmi | |||
|