

|
|||||||||
AbstractAnkyloglossia is a congenital oral anomaly characterized by an abnormally short lingual frenulum. Ankyloglossia is less common in adults as compared to infants. Sialolithiasis usually occurs between the third and fifth decades of life. The submandibular gland is the most frequently involved salivary gland. This is the first case of ankyloglossia accompanying sialolithiasis in literature which we could access. If ankyloglossia is left untreated for a long time, this condition may cause submandibular sialolithiasis. Therefore in ankyloglossia treatment, submandibular sialolithiasis must be considered.IntroductionThe incidence of ankyloglossia has been reported between 0.02% and 10.7% [1]. In adolescents or adults the prevalence ranges from 0.1% to 2.08%. Ankyloglossia affects males more commonly [2]. Ankyloglossia is a congenital oral anomaly characterized by an abnormally short lingual frenulum [3]. Ankyloglossia is characterized by short vertical length of the lingual frenulum, which may result in a varying degree of decreased tongue tip mobility [4]. Ankyloglossia is less common in adults as compared to infants and some authors have hypothesized that ankyloglossia improves with age [3]. The clinical consequences of ankyloglossia include infant breastfeeding difficulties, speech disorders, various mechanical and social issues related to disability of tongue movement, and orthodontic anomalies [4]. About 79 % of salivary calculi are in the submandibular glands and 34% of them are localized in the duct of Wharton’s, 57% in the hilum and 9% inside the gland [5,6]. Sialolithiasis usually occurs from the third to fifth decades of life, and is slightly more often in males [7]. The submandibular gland is the most frequently involved salivary gland because of the longer length of its major duct with a narrow orifice, as well as the nature of the submandibular gland secretion, which can have a consistency as thick as a gel [8]. This gel becomes a framework for deposition of salts, which leads to development of calculi [9]. Small calculi of approximately 3–7 mm are common either in the submandibular duct or gland. Single giant calculus of size 33 mm [9] 10 mm in the submandibular duct or multiple calculi of 7 in number of an average diameter of 7–8 mm within the submandibular gland are extremely rare 10. Case ReportA 17-year-old teenager presented to our clinic with compliants of a sublingual swelling for 3 months and pus discharge from the left Wharton's papilla of 2 weeks duration (Figure 1).
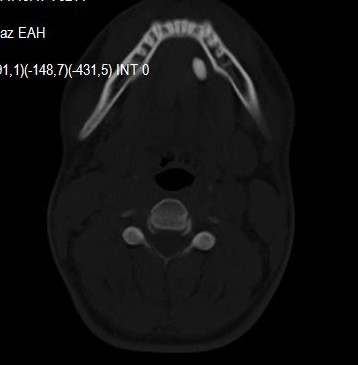
The patient’s history revealed previous recurrent left submandibular swelling and pain after eating. In oral examination, there was a short lingual frenulum and a swelling of 1x1 cm dimension in the left sublingual region. On the cervical CT scan, a hyperdense lesion of 11 mm diameter was observed in the left sublingual region (Figure 2).
The patient underwent frenuloplasty and transoral excision of the calculus in the left Wharton’s duct. (Figure 3)
The dimensions of the calculus were approximately 20x10 mm (Figure 4).
DiscussionPredisposing factors for submandibular sialolithiasis are salivary stasis, increased alkalinity of the saliva, infections of the oral cavity, physical trauma to the submandibular duct or gland, smoking, and diuretic use [10,11]. Ankyloglossia or tongue-tie is a short attachment of the lingual frenulum. The lingual frenulum connects the ventral tongue to the floor of the mouth. In the case of a short lingual frenulum, forward and downward pressure of the tongue to the mandible may cause growth of the mandible in a more prognathic manner and different consequences on face development [4,12,13]. Also, the increased pressure of the tongue may lead to a decrease or even halt of the submandibular salivary flow. The incidence of ankyloglossia is low in adults [2]. Submandibular sialolithiasis may be seen in children also with low incidence, since relatively long time is required for the formation of a salivary calculus, and sublingual papilla is very small in children, which blocks the ingress of foreign material required for the initial nidus formation. However, a calculus is formed more easily in adults than in children [9]. Although submandibular sialoliths are usually asymptomatic, pain and swelling which increase with food anticipation may be the cardinal signs and symptoms [9,14,15]. The presented case was a teenager who had ankyloglossia and an intraductal sialolith. This is infrequent in teenager. Although CT, magnetic resonance imaging, and X-ray can be used to diagnose sialolithiasis, the most effective diagnostic imaging modality is sonography [16]. In our case CT was preferred. Surgical repair may be considered in patients with a tight lingual frenulum, as outlined below, and a history of associated feeding, speech, or mechanical/social difficulties. The diagnosis of ankyloglossia is confirmed by characteristic examination findings. The tongue is often heart-shaped at its tip. Tongue protrusion is limited, and the tip may not extend past the lower lip. When the tongue protrudes past the teeth, the midportion of the tongue typically rolls or curls forward, but the tip itself is drawn inferiorly by the frenulum with little forward extension. Tongue elevation is also characteristically impaired. Frenuloplasty and frenotomy are the most commonly used surgical procedures for treatment of ankyloglossia [17]. The primary treatment of submandibular sialolihiasis consists of stimulation of saliva production and massage of the gland. The other treatments include submandibular gland excision, sialoendoscopy or transoral removal of the calculi [6,18]. Surgical treatment for the submandibular calculi is chosen according to location and palpability of the sialolith. Intraoral removal is more suitable for sialoliths which are palpable in the mouth and are located in the distal duct at a distance of no more than 2 cm from the ostium of Wharton’s duct [19]. Intraoral excision of the ductal calculi is managed with linear incision on the mucosa along the duct on the place of the calculus bulge and is removed [10]. In our case, firstly frenuloplasty was perfprmed, followed by intraoral excision of the ductal sialolith. To our knowledge, this is the first case of ankyloglossia accompanying sialolithiasis in the accessible literature. If ankyloglossia is not treated for a long time, this condition may cause submandibular sialolithiasis. Therefore in ankyloglossia treatment, submandibular sialolithiasis must be considered. References
|
|||||||||
| Keywords : Ankloglossi , submandibuler , sialolitiazis , submandibuler sialolitiazis | |||||||||




|