

Authors
|
|||||||||||||
AbstractFrontal sinus drainage is associated with embryological development. Drainage is usually direct or by way of rudimentary anterior ethmoid cells into the frontal recess. The frontal recess is a deep recess in the anterosuperior part of the middle meatus. A closed duct, known as the frontonasal duct (FD), forms in the upper surface of this recess. Narrowing and obstruction of the FD leads to compromise of frontal sinus drainage and to sinusitis. Frontal sinus infection may lead to osteitis in the front wall. If it spreads from there, it may result in pus accumulation beneath the frontal periosteum, known as Pott’s puffy tumor. We present a case of polyp causing isolated, unilateral, complicated, acute frontal sinusitis by obstructing the FD. To the best of our knowledge, this is first such report in the literature.IntroductionThe anterior ethmoid, maxillary and frontal sinuses drain into a region known as the osteomeatal complex in the middle meatus. Narrowing in the osteomeatal complex creates a preparatory environment for sinusitis. Frontal sinus drainage is associated with embryological development. Drainage is usually direct or by way of rudimentary anterior ethmoid cells into the frontal recess. This is a deep recess in the anterosuperior part of the middle meatus. A closed duct, known as the frontonasal duct (FD), forms in the upper surface of this recess. Narrowing and obstruction of the FD leads to compromise of frontal sinus drainage and to sinusitis [1]. Frontal sinus infection may lead to osteitis in the front wall. If the infection spreads from there, it may cause pus accumulation beneath the frontal periosteum, known as Pott’s puffy tumor [2]. We describe a very rare case of complicated, unilateral, acute frontal sinusitis of polyp origin obstructing the mouth of the FD in the intranasal region. Case Report
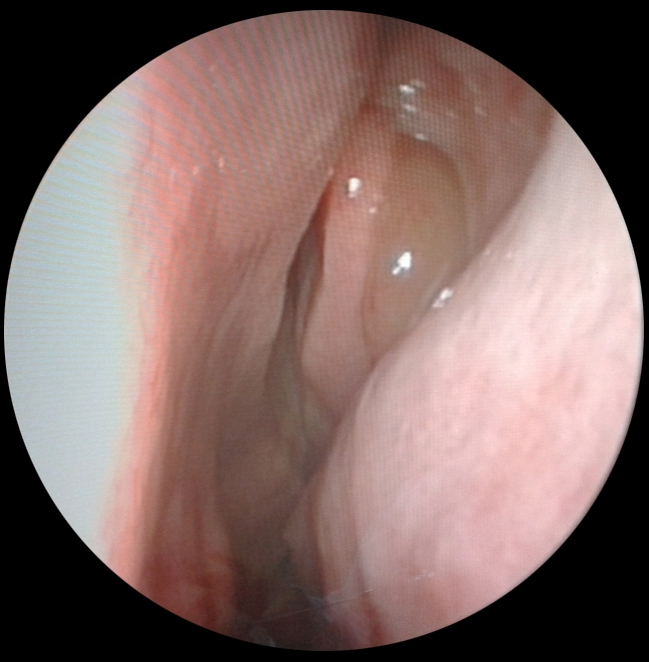
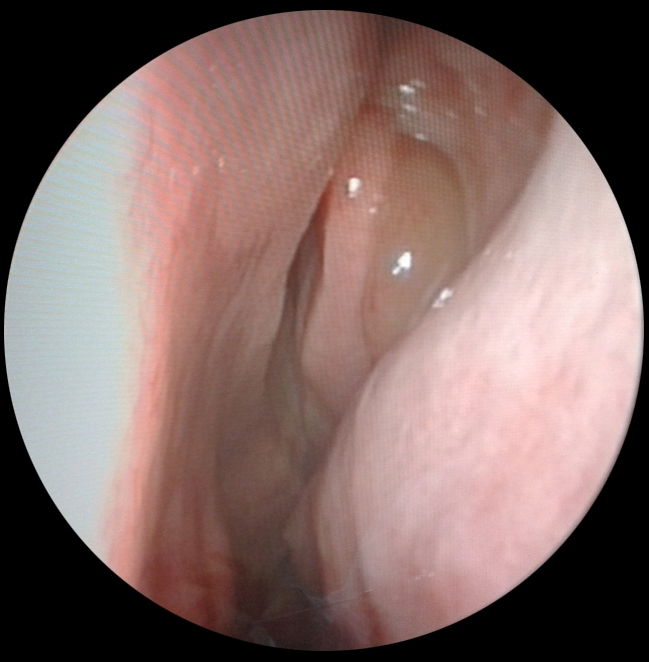
Our patient was a 36-year-old man with headache persisting for the previous 15 days despite the use of drugs and a painful and increasing swelling above the left eyebrow. There was no story previously passed a nasal or sinus surgery and trauma at the case. In the patient, chronic sinusitis and history of allergy was not available. Clinical examination revealed only a small polyp in the left frontal recess (Figure 1) and sensitivity and expansion at palpation in the left frontal sinus anterior wall.
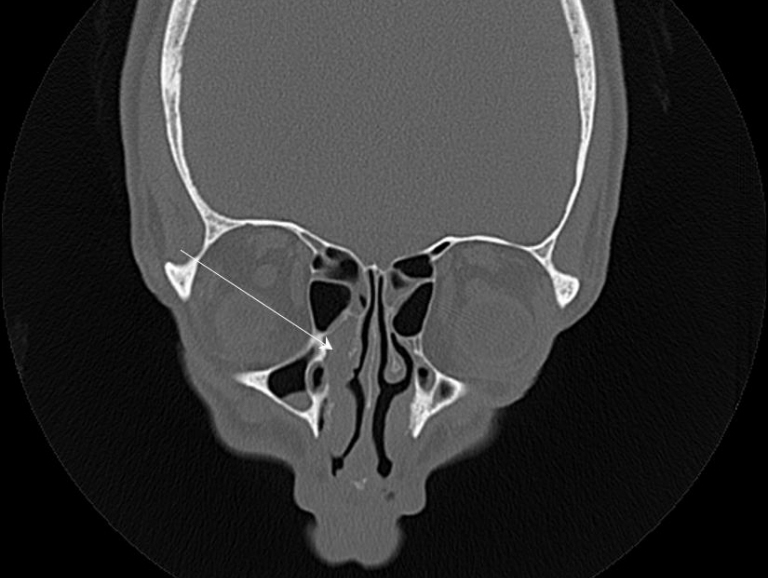
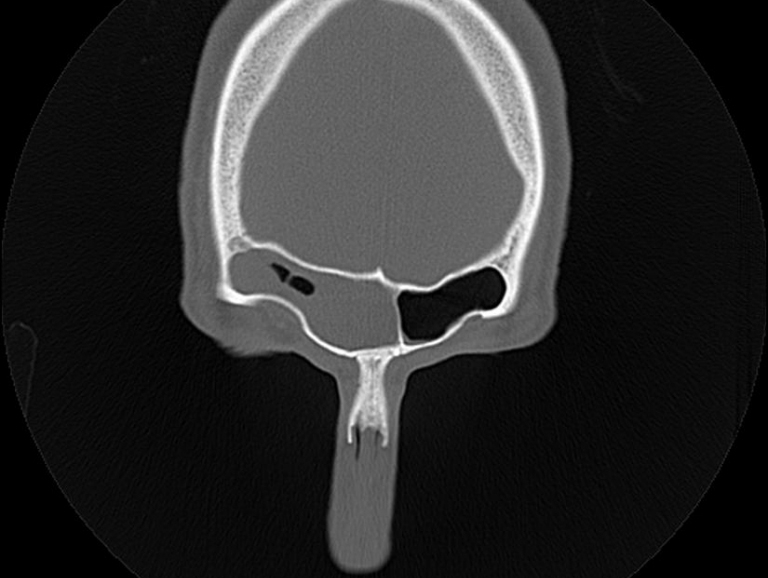
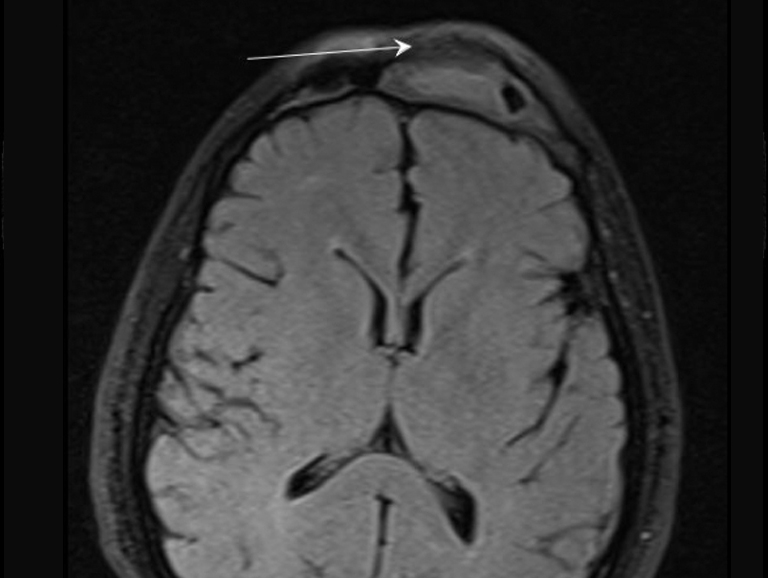
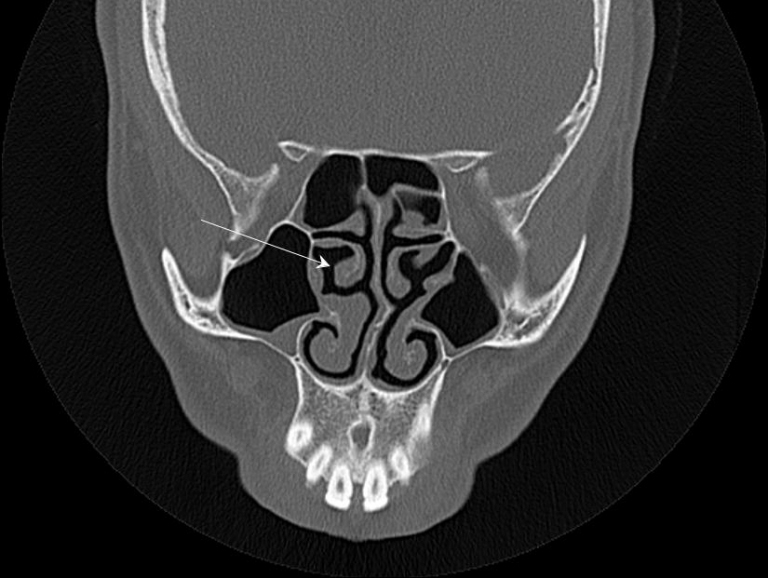
Paranasal sinus tomography and magnetic resonance imaging revealed a polyp obliterating the left FD (Figure 2) and the presence of unilateral sinusitis in the left frontal sinus (Figure 3) and of Pott’s puffy tumor at the front of anterior wall of the left frontal sinus (Figure 4-5). No polypoid tissue was observed anywhere other than in the left frontal recess (Figure 6). Endoscopic sinus surgery was performed, and the intranasal polypoid tissue and pus filling the frontal sinus were completely removed. No problems or recurrence were observed at 3-month follow-up. DiscussionThe inflammatory polyp is thought to be a membrane hyperplasia caused by chronic inflammation. This pathology is usually allergic in origin, and is most commonly located in the nasal cavity or maxillary sinus. At computed tomography (CT) it is typically observed as a homogeneous soft-tissue mass. When severe, polyps may cause obstruction, leading to the accumulation of secretions and expansion of the sinus walls. At this point, the pathology may resemble tumors, and differentiation at CT becomes difficult [1].Our case involved a polyp obstructing the mouth of the FD at the left frontal recess, resulting in sinusitis and expansion in the left frontal sinus. Paranasal sinus tomography should be used in treatment-resistant sinuses, in patients who may require surgical intervention and in the presence of complications. Nasal polyposis and acute complicated sinusitis are among the definitive indications for surgery [3]. Paranasal sinus endoscopy can be performed as a diagnostic procedure or as a therapeutic procedure (functional) to clear obstructed sinus ostia. “Functional” endoscopic sinus surgery is usually used for patients in whom medical treatment fails and who have disease of the osteomeatal unit shown by CT or diagnostic endoscopy [4]. The advantages of functional endoscopic surgery include more accurate diagnosis of malformations or obstructing masses causing refractory sinusitis [5], and precise localization and removal of the site of disease with mucosal preservation and restoration of normal mucociliary drainage [6]. Osteomyelitis is a regional complication of sinus inflammation and most commonly occurs in the frontal bone [7]. Infection in the sinus can spread hematogenously, via diploic veins, or by direct extension. Intensive treatment is required. Frontal bone osteomyelitis, known as Pott’s puffy tumor, causes lytic destruction of the frontal bone associated with an extracranial soft tissue mass [8]. Pott’s puffy tumor, an untreated frontal sinusitis, usually leads to osteomyelitis of the anterior wall of the frontal sinus and subperiosteal abscess formation. The anterior wall of the frontal sinus is thinner than the posterior wall and is more sensitive to abscess formation [9]. Relationship between intracranial complication with Pott’s puffy tumor is regarded to be high. The intracranial complications have been observed 67% of patients with Pott’s puffy tumor [10]. There wasn't any intracranial complication in our case. Pott’s puffy tumor is a surgical emergency. Traditionally surgical treatment of Pott's puffy tumor is external approach . It provides direct visualization of pathologic area on the frontal sinus, but this procedure can do cosmetically unfavorable facial scars [11]. Treatment with modern functional endoscopic sinus surgery can usually be performed with minimal invasion [12]. Only a few case reports have described the use of endoscopes in the treatment of Pott’s puffy tumor. This is due to the complex anatomy of the frontal recess and to endoscopic surgery still being controversial in this region [11]. In our case, frontal recess polyp, unilateral left frontal sinusitis and Pott's puffy tumor were successfully treated using endoscopic sinus surgery. In conclusion, patients with single-sided, isolated, complicated sinusitis should receive endoscopic examination. CT should be performed, and emergency endoscopic surgical intervention should be considered. We present a case of polyp causing isolated, unilateral, complicated, acute frontal sinusitis by obstructing the FD, the first such case according to our review of the literature. References
Presented at11th International Congress of ENT, Ankara, April 2014 |
|||||||||||||
| Keywords : Frontal Sinüzit , Polip , Pott’ un puffy tümörü | |||||||||||||

|