

Authors
|
|||||||||||
AbstractThe metastasis of colorectal cancers to the maxillofacial region is extremely rare, but its prognosis is poor. Metastasis to the maxillofacial bones mostly occurs in the molar region of the mandible. Metastasis from the colon region to the zygoma region is limited to a single case in the literature. This paper outlines the case of a 68-year-old female patient presenting with swelling and pain in the right zygoma region whose colon adenocarcinoma metastasis was detected in a biopsy. The first signs of tumors outside the head and neck region may encompass metastasis in the maxillofacial region, so swelling and pain in the facial area should be suspected .IntroductionMetastases to the skin, soft tissue, and bones of the maxillofacial region are extremely rare, but they can occur from the breast, lung, kidney, thyroid gland, digestive system, and prostate [1,2]. Such metastases are usually found in the molar region of the mandible [2]. The prognosis of metastases from tumors outside the head and neck region to the maxillofacial region is quite poor [2,3], and life expectancy in such cases is less than one year [2]. Since metastases to the maxillofacial region are uncommon, a sufficient number of cases could not be found to assess effective fixed treatment protocols. Metastases to the zygoma, a maxillofacial sub-region, are limited to a few case reports in the literature. While colorectal tumors are common [4], the metastases of such cancers primarily occur in the liver and lung regions [4], and their metastasis to the maxillofacial region is particularly rare. A single case of colorectal cancer metastasizing to the zygoma region was found in the literature review [4]. Case ReportA 68-year-old female was initially hospitalized for abdominal pain in 2016 and a hemicolectomy was performed. A microscopic examination revealed colonic-type adenocarcinoma beginning from the mucosal surface and infiltrating all layers of the colon. She went through 12 cycles of FOLFOX (folinic acid, fluorouracil and oxaliplatin) chemotherapy after the cancer metastasized to 44 lymph nodes. In July 2017, she presented with pain and swelling in the right zygomatic arc area (Figure 1)
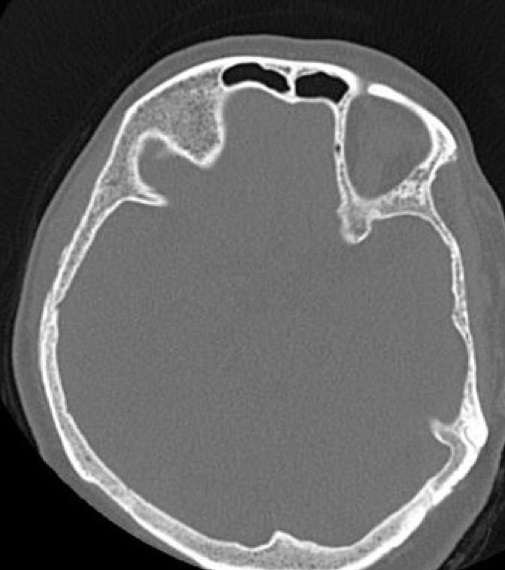
The patient was followed up with when a ground glass image compatible with fibrous dysplasia was reported in a CT scan of the paranasal sinus (Figures 2 and 3).
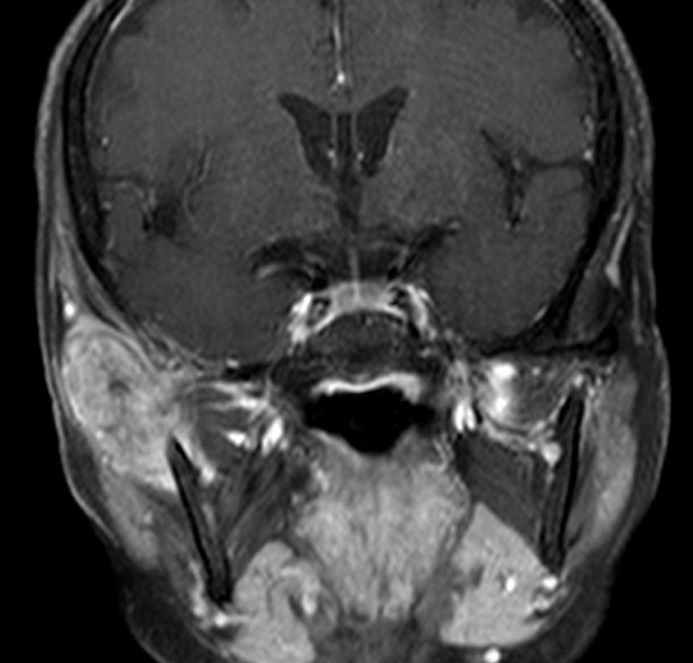
An MRI was performed due to increased complaints of pain and swelling. The MRI showed a mass lesion with a chondroid matrix appearance of 37 x 24 mm in the largest area extending from the zygomatic arch level to the right masseter muscle (Figure 4).
A biopsy was performed following the MRI results. In September 2017, an incisional biopsy was performed and the histopathology showed adenocarcinoma metastasis (Figure 5).
A PET-CT scan performed on the patient revealed metastasis in the zygoma region and lung . In October 2017, the patient was prescribed FOLFIRI + CETUKSIMAB for 18 cycles every 14 days (Irinotecan 180 mg / m[2], Folinic acid 200 mg / m[2], 5-FU 2600 mg / m[2], Cetuximab 500 mg / m[2]). Treatment was stopped when stable findings appeared on PET-CT scans. The patient died in the 19th month after starting treatment. DiscussionThe metastasis of cancers far from the oral and maxillofacial region characterize only 1% of cancers in this region [2]. Metastases usually occur after the age of 60, 20% of which are detected before the primary tumor [2,5], following which many patients die within a few months to a year [5]. Masakatsu et al. [2] retrospectively evaluated nine patients with maxillofacial metastasis . Only one of the patients had zygoma metastasis. In six patients with metastasized cancer, including zygoma metastases, they found that the primary tumors were outside the head and neck region in all six patients. The first complaints of these six patients occurred in the head and neck region. They detected metastasis in the zygoma region from primary adenocarcinoma of the stomach. The patient who underwent chemotherapy lived for about 6 months . In the retrospective study of 1,221 patients with maxillofacial or oral cancers, Shown et al. [1] detected metastatic tumors in only 26 patients. Among 25 patients , primary adenocarcinoma in the head and neck region was found in 34.6% of cases. In one patient, the primary cancer could not be detected. In this study, metastasis was detected before the primary tumor in 62% of patients, but no metastasis to the zygoma region was detected. Only three patients exhibited primary colon and histologic adenocarcinoma. Common symptoms of metastatic tumors in the maxillofacial region are asymmetry, swelling, pain, and loss of sensation in the face. The first sign of tumors outside the head and neck region may be metastasis to the maxillofacial region. It is difficult to clinically diagnose patients who first present with swelling and redness in the maxillofacial region [6]; these symptoms are often confused with infection, in which case antibiotics are usually preferred as the first treatment. This should be kept in mind for patients presenting with such complaints, and more care should be taken for patients whose complaints continue despite treatment. After our patient’s complaints of pain and swelling did not disappear, we conducted a biopsy based on MRI results. After CT scan results, we followed up with the patient to report a diagnosis of fibrous dysplasia. When left untreated, some metastases causing pain and swelling can present in the facial region. Colorectal cancers are among the most common cancers , the pathological diagnoses of which are most often adenocarcinoma[4]. The US sees 150,000,000 new cases of colorectal cancer per year with an estimated 60,000 deaths [4]. Colorectal cancer metastases are indicative of poor prognosis and often occur in the liver, lungs, peritoneum, bones, and ovaries [4]. Rare metastasis sites are also presented in the literature. These include the larynx, tongue root, and brain [4]. Metastases to the maxillofacial region are limited to very few case reports. When we reviewed the literature, we encountered only nine case reports of metastasis to the malar region. These occurred from the thyroid [7], breast [3], lungs [8,9], liver [10,11], cervix [12], rectum [4], and stomach [2]. Malar metastasis from the rectal region of the colon was reported in only one case [4]. In the only case of zygoma metastasis where the primary tumor was colon adenocarcinoma, radiotherapy was applied after metastasis was detected and the patient died two months later. Our patient was given cetuximab in combination with chemotherapy with an estimated a 19-month life expectancy. While anti-epidermal growth factor receptor (EGFR) antibodies are widely used in metastasized colon cancers [13], larger-scale studies are needed to substantiate their effectiveness [14]. We found it appropriate to add cetuximab due to its use in colon metastases and the poor prognosis of maxillofacial metastases . We believe we obtained better results than in similar case reports. References
|
|||||||||||
| Keywords : Zigomatik metastaz , kolorektal kanser , anti epidermal büyüme faktörü | |||||||||||




Login to write a comment.
|
|