

Authors
|
|||||||||
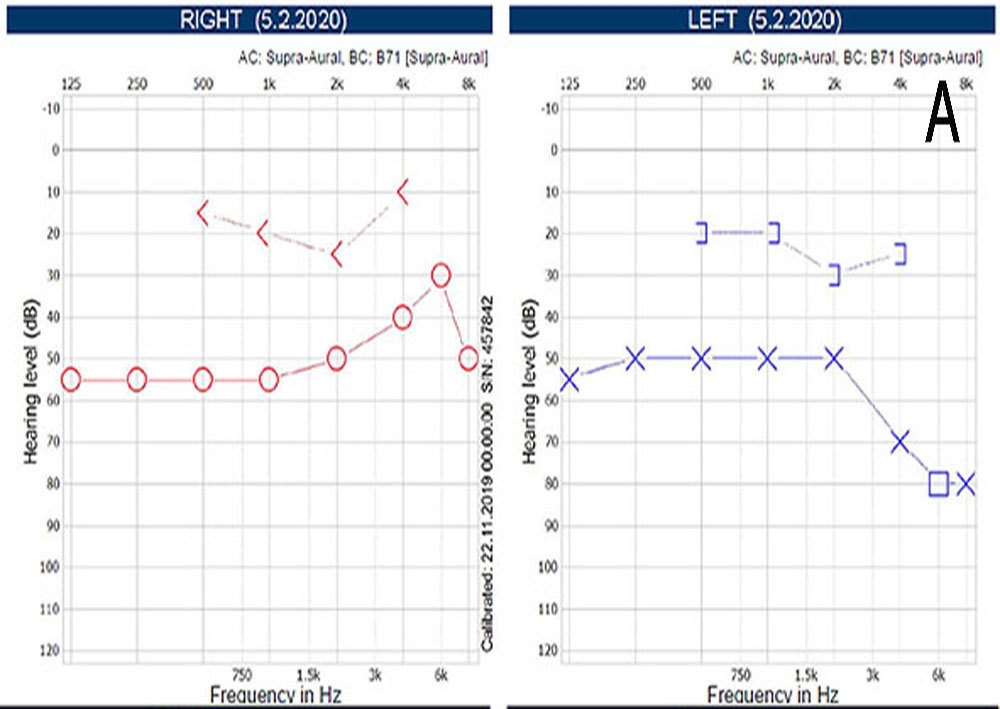
AbstractOtosclerosis is one of the pathologies frequently observed in otolaryngology clinics. The most common pathology in this disease is fixation of the stapes footplate. In its clinic, it is frequently encountered as progressive conductive hearing loss. When exploratory tympanotomy is performed for the diagnosis and treatment of otosclerosis, rare pathologies such as incudomalleolar fixation, stapes tendon fixation, stapes suprastructure fractures, and incudostapedial dislocation might be found as the cause of conductive hearing loss. One of these pathologies, the long process of incus (LPI) defects seen during the otosclerosis surgery, are most frequently encountered in revision surgeries performed for unsuccessful stapedectomy operations. In this case report, we present a primary otosclerosis case with LPI defect and no previous history of surgery, infection or trauma. The case we present is the first report of a primary otosclerosis with LPI defect in the literature. It should be taken into consideration that patients scheduled for primary otosclerosis surgery may have an incus defect.IntroductionOtosclerosis is frequently observed in otolaryngology clinics associated with complaint of conductive hearing loss. It is mainly surgically treated with stapedotomy. It is also accurately diagnosed through surgical and pathologic examinations. However, rare pathologies such as incudomalleolar fixation, stapes tendon fixation, stapes suprastructure fractures, and incudostapedial dislocation, with clinical symptoms similar to otosclerosis, may be encountered intraoperatively [1]. One of these pathologies, the long process of incus (LPI) defects seen during the otosclerosis surgery, are most frequently encountered in revision surgeries performed for unsuccessful stapedectomy operations. We present the case of primary otosclerosis with LPI defect, without previous history of surgery, infection or trauma. To the best of our knowledge, LPI defect that causes incudostapedial dislocation accompanied with primary otosclerosis has not yet been previously reported in literature. Case ReportA 44-year-old female patient attended to our clinic with complaints of bilateral hearing loss that started 20 years ago. No history of previous ear surgery, ear infection, head and neck or systemic trauma, and similar complaints in her family were found in the patient’s anamnesis. In the physical examination, tympanic membranes were intact and normal. On the pure tone audiogram , the patient had bilateral mild mixed hearing loss: left air bone threshold, 52/23 dB; right air bone threshold, 51/27 dB. Furthermore, Carhart’s notch, suggesting otosclerosis, was observed bilaterally (Figure 1).
The “As” curve was observed in the tympanometry, and bilateral stapes reflexes could not be obtained. The thin section temporal bone computed tomography was reported as normal. In accordance with these findings, an explorative tympanotomy was planned for the preliminary diagnosis of otosclerosis in the left ear (Video 1).
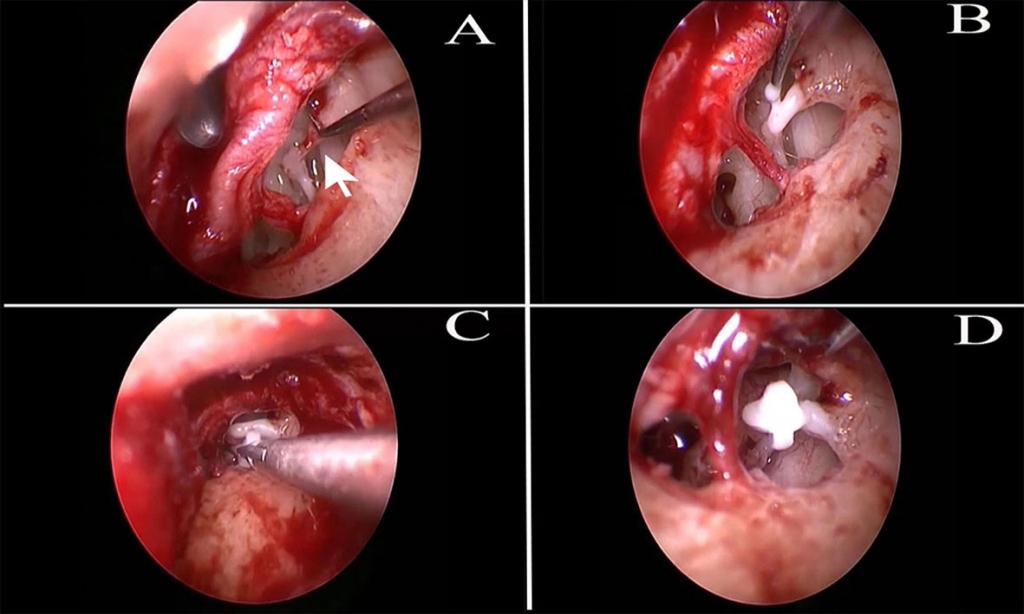
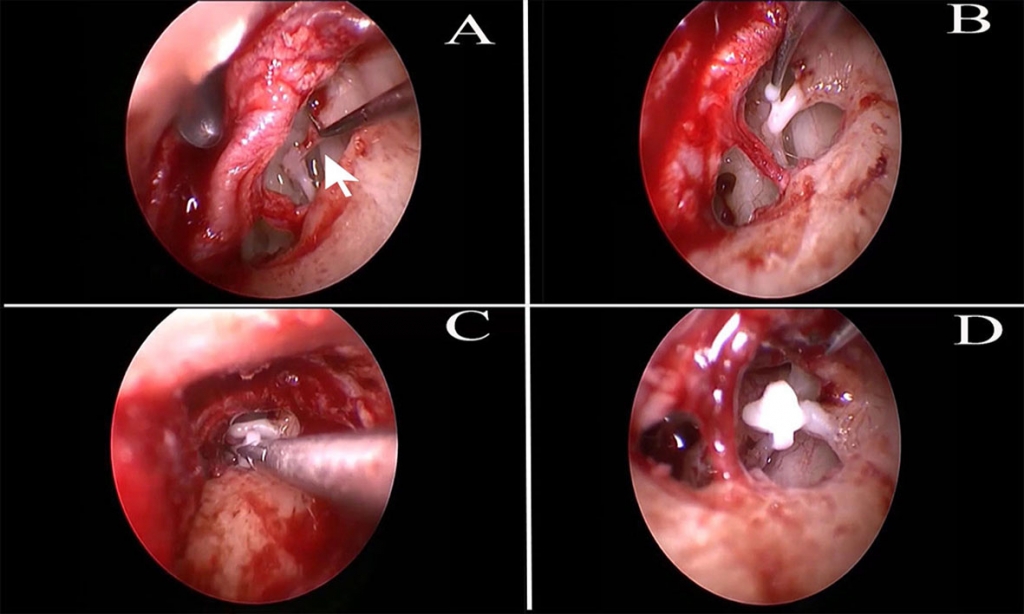
When ossicles were visualized, a 2–3-mm defect on LPI that leads to incudostapedial dislocation was revealed. However, the lenticular process of the incus was found intact over the stapes suprastructure (Figure 2A). In conclusion, the patient was confirmed to have primary otosclerosis with LPI defect that causes incudostapedial dislocation. Afterward, LPI defect was reconstructed with Otomimix (Walter Lorenz Surgical Inc, Jacksonville, FL) Hydroxyapatite Bone Cement (HBC) and the incudostapedial connection was obtained (Figure 2B). After 10 min of waiting for cement hardening, 4[3/4 ]mm-long Teflon piston (Audio Technologies SRL, Piacenza, ITALY) was inserted to the stapedotomy hole and attached to the reconstructed HBC (Figure 2C). To prevent the risk of prosthesis dislocation from reconstructed incus, a small drop of cement was used to fix the Teflon piston to the reconstructed LPI (Figure 2D).
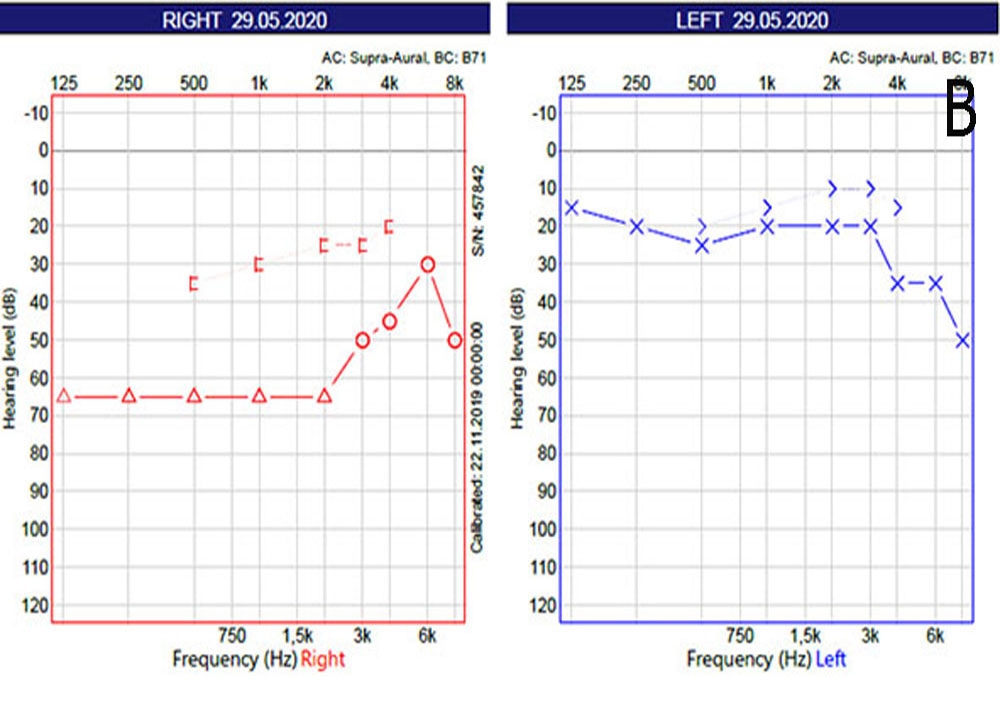
Thereafter, the ossicle system’s mobility was confirmed. In the postoperative 12 week, pure tone audiogram was found to be 21/15 dB and air-bone gap was 6 dB in the patient’s left ear (Figure 3). Informed consent was obtained from the patient who participated in this case.
DiscussionThe prevalence of clinical otosclerosis is 0.3–0.4% in the general population [2]. It's certain diagnosis is obtained by revealing the stapes footplate fixation with explorative tympanotomy and pathologic examination. However, when explorative tympanotomy was performed for otosclerosis, rare pathologies such as incudomalleolar fixation, stapes tendon fixation, stapes suprastructure fractures, and incudostapedial dislocation might be found as the cause of conductive hearing loss [1]. One of these pathologies, LPI defects seen during the otosclerosis surgery, are most frequently encountered in revision surgeries performed for unsuccessful stapedectomy operations [3]. In these studies, various techniques such as establishing a connection of vestibule with the defective LPI arm with various prosthesis, performing a malleostapedotomy bypassing the defective incus, and placing total ossicular replacement prosthesis (TORP) by bypassing the ossicles have been attempted [4,5]. However with the increasing popularity of cements in otolaryngology practice due to its easy, fast, reshape able, cheap, and biocompatible properties, it has been frequently used in otologic surgeries especially for the treatment of incudostapedial dislocations. In our clinic, we use HBC which was shown to be a more biocompatible, bio-stable, and well tolerated by bone and soft tissues in previous studies [6]. In order to especially prevent the risk of cement leakage into the inner ear via an opened vestibule that would be performed for stapedectomy, LPI reconstruction was firstly performed in this case and a 10-min waiting time was allowed for complete hardening of the cement before stapedectomy. Van Rompaey et al. compared the application of the malleovestibular (MV) prosthesis with stabilization of the new piston to the defective LPI with HBC application in revision stapes surgeries. They reported that both groups have similar success on postoperative air-bone gap closure [7]. Chen et al. performed revision stapes surgery to 7 patients who had the LPI defect. In 6 patients, they fixed the prosthesis to the defective LPI and in one patient; they attached the new prosthesis to the reconstructed LPI by glass ionomer cement. They reported that hearing results of the prosthesis inserted to newly reconstructed LPI with cement were less successful [8]. This application is similar to that of our procedure; however, as the authors indicated, their failure is related to the improper application of the cement. They proposed to extend the 10-min waiting time for to dry to prevent this failure. In these previous studies, fixing the prosthesis to the incus remnant revealed favorable results. However, this application is associated with risks of cement leakage to the vestibule, prosthesis dislocation, and mechanical trauma to the inner ear during the stabilization of prosthesis until the cement hardens [7]. Therefore, LPI reconstruction should be performed with cement primarily in these cases, and then performing stapedectomy prevents these risks. Another advantage of reconstructing the LPI rather than fixing the prosthesis to the remnant incus is obtaining a neutral anatomic position of the ossicles and the hearing physiology. In normal hearing physiology, the incus length ratio to the malleus length is 1.3, facilitating an increased acoustic energy transmitted to the inner ear from the ossicles. In our technique, restoring the incus to its own length using cement and attaching the prosthesis to it allows advantages of acoustic energy increment by obtaining neutral incus/malleus ratio. Furthermore, using this technique, the piston’s entering angle to the vestibule is more similar to the neutral stapes position. However, obtaining these advantages by fixing the prosthesis to the incus remnant is impossible in the application of TORP or MV prosthesis. However, although we did not observe any intraoperative complications and air-bone gap was almost completely closed postoperatively, this application might have additional risks in terms of hearing results by restricting the movement of the prosthesis and increasing the mass of the ossicles over the vestibule and still having the possible risk of cement leakage to the opened vestibule. Accordingly, further studies should be performed to clarify the need of prosthetic fixation to the reconstructed incus with cement. In conclusion, to our knowledge, we firstly report a case of primary otosclerosis with a LPI defect that causes incudostapedial dislocation and its successful treatment with HBC. In cases like ours, this surgical procedure is found to be favorable according to its ease of application, lower risk of vestibule trauma, neutral anatomy closer of the ossicles and piston entering angle to the vestibule. References
|
|||||||||
| Keywords : Otoskleroz , inkus defekti , stapedektomi , kemik çimentosu | |||||||||

|