

Authors
|
|||||
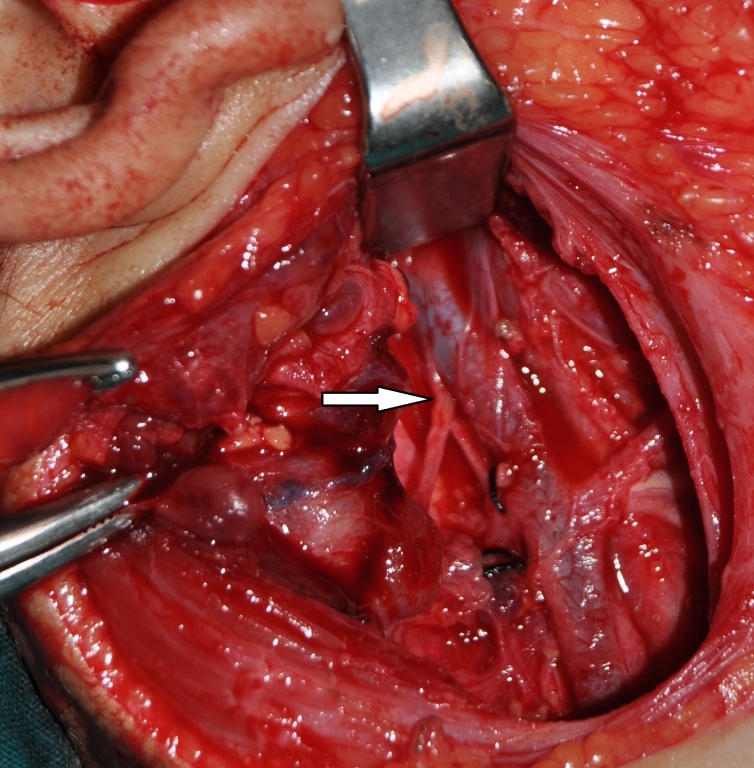
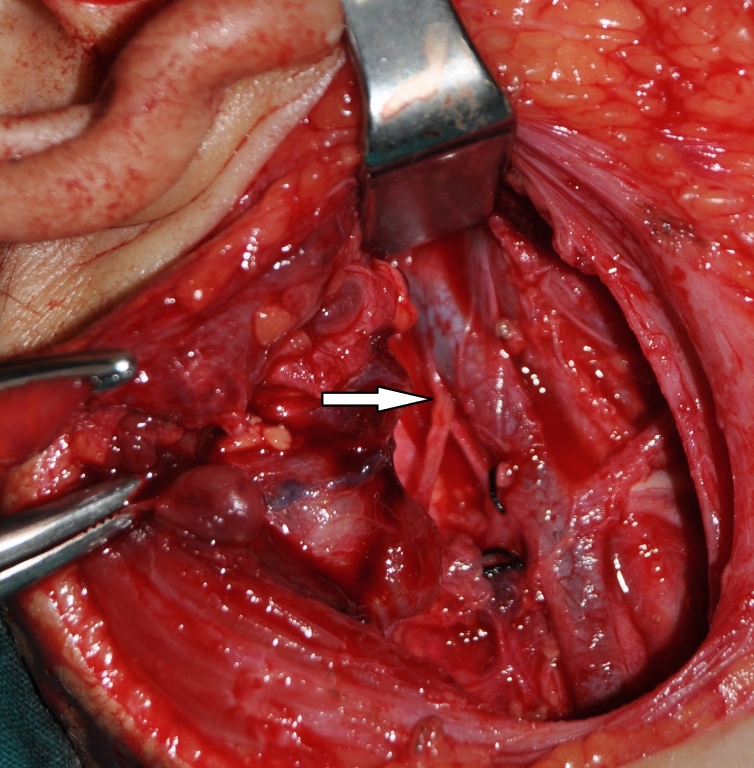
AbstractDuring surgical intervention dealing with level II; the most important anatomical structure is spinal accessory nerve. The anatomic relationship between spinal accessory nerve with internal jugular vein in this level is very important for precluding neurovascular complications. The nerve mostly passes lateral( anterior) or medial( posterior) to internal jugular vein at the level of medial aspect of posterior belly of digastric muscle. Very few cases of spinal accessory nerve passing through a fenestrated internal jugular vein are published. Most of these cases are cadavers or neck dissection results of a known aerodigestive malignancy. We presented the first case of 4 years old patient with a parotid region lymphangioma descending to level II with a spinal accessory nerve passing through the fenestrated internal jugular vein. Anatomic variations between spinal accessory nerve and internal jugular vein are discussed with their clinical impacts under the light of current literature.IntroductionLevel II is the regional lymph node group descending from skull base to bifurcation of carotid artery or the hyoid bone. Anterior limit of this region is sternohyoid muscle and posterior limit is posterior border of sternocleidomastoid muscle. The most important anatomical structure in this region is spinal accessory nerve (SAN). Lymph nodes anterior to SAN are designated as level IIA, whereas lymph nodes posterior to this nerve belong to level IIB [1]. During surgical intervention in this region such as a neck dissection; anatomical course of SAN must be known. Although variable anatomic relationships between the nerve and internal jugular vein (IJV) exist in the literature, SAN mostly passes anterior( lateral) to IJV and less commonly posterior ( medial) to it [2-4]. A few cases of SAN passing through a fenestrated IJV are also published [2-8]. Most of these were neck dissections for a known malignancy or cadaveric studies. We presented the first case of SAN passing through a fenestrated IJV in a pediatric patient during neck exploration of level II for a benign neck mass lymphangioma (LAM). Case ReportFour years old otherwise healthy girl was consulted to our Mersin University Otorhinolaryngology department from Plastic and Reconstructive surgery for mass in the right upper neck. In her medical history the mass was learned to be present in the newborn period and gradually increased in size descending to neck region. In her physical examination; a 4 x 4 cm. tender mass starting from preauricular region descending to right level II was palpated. On her neck and parotid computerized tomography; an irregular shaped mass starting from preauricular region descending to thyroid cartilage level with involvement of the right parotid gland was seen with the preliminary diagnosis of lymphangioma. Superficial parotidectomy with neck exploration was performed under general anesthesia. During surgical intervention in the upper neck posterior belly of the digastric muscle was extracted to be able to totally excise the mass in the level II. After extraction of the muscle, an unusual anatomic relationship between SAN and IJV was seen. The IJV had a fenestration nearly 1 cm. above the carotid bifurcation. The nerve transmitted through the fenestrated IJV. ( Figure 1)
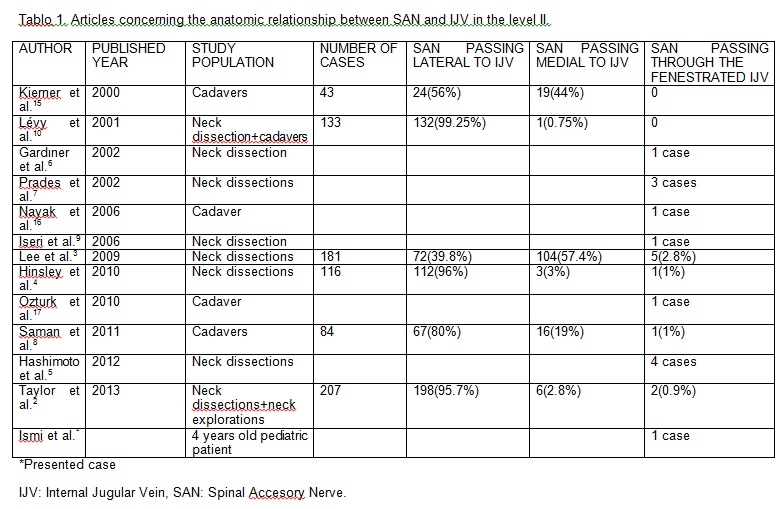
Superficial parotidectomy was performed with neck exploration and the mass was totally excised. Postoperative pathological analysis of the specimen resulted as lymphangioma. Postoperative period was uneventful without complication, there was no facial weakness or shoulder pain and the patient was discharged on the fourth day. DiscussionSpinal accessory nerve is the XIth cranial nerve which exists the cranium through jugular foramen with other nerves glossopharyngeus and vagus. It passes mostly lateral or medial to IJV before giving rise to motor innervation of sternocleidomastoid and trapezius muscles. It courses neck level II in a superoinferior and medial to lateral direction dividing the space into two as level IIA and IIB [3]. It has several anatomic connections with other cervical and cranial nerves, the term spinal accessory nerve plexus was used to describe this condition [9]. During surgical manipulation in level II, traumatic injury to SAN can cause shoulder syndrome which is characterized by shoulder pain, limited movement and dropping of the shoulder which has adverse effects on quality of life of the patients [3]. To avoid shoulder syndrome and vascular damage to IJV, anatomic relationships and variations between SAN and IJV must be well known. There are great variations among authors for anatomic relationship of SAN and IJV. In the series of Lee et al. SAN passes IJV ventrally (anterior) in 39.8 % of cases, dorsally (posterior) in 57.4 % of cases. There was only 2.8 % of cases SAN passes through the fenestrated IJV like our case [3]. For Taylor et al. lateral(anterior) crossing was 95.6% and medial (posterior) crossing was 2.8%. SAN passing through the fenestrated IJV was only 0.9 % of cases [2]. For Saman et al. with cadaver series SAN crossed IJV anteriorly in 80 %, posteriorly in 19 % of cases. Only one case (1%) was present with SAN piercing the bifurcated IJV [8]. Recently Hinsley and Hartig presented a neck dissection series with a dominant lateral crossing type.(96%) SAN crossing through the fenestrated IJV was only 1 % in their series. [4] Levy et al. studied 123 neck dissection patients with addition to 5 cadavers, none of them showed a SAN passing through the fenestrated IJV [10] The articles concerning the anatomic relationship between SAN and IJV were summarized in table 1. The great variations regarding the ratios of anatomic relationship between SAN and IJV can be explained by study population and level of dissection. In the cadavers the tissues are shrunken and IJV may be collapsed which modifies the relationship with SAN. This condition may explain a higher incidence of SAN medial (posterior) crossing to IJV at level II in cadaver studies [10]. Also if the dissection is not carried out high enough at the level of medial aspect of digastric muscle, the nerve may falsely seem to lie posterior to the vein which also contributes to false positive result of a medially crossing nerve [2]. The terms fenestration and duplication were used interchangeably by authors for describing the accessory lumen of IJV. Downie et al. suggested a new classification, they argued that the term duplication should be used for cases of IJV joining the subclavian vein as separate two veins in an up-side-down Y pattern. They also mentioned that the term fenestration should be used for cases who have IJV branching into two veins for some distance, the veins refuse and enter the subclavian vein as a single vein like our case [11]. When a fenestrated IJV exists, mostly SAN passes through the fenestration [5]. Rarely SAN can pass medial (posterior) part of the fenestrated IJV [12]. The exact cause of a SAN passing through the fenestrated IJV is not known, but mostly an embryological base is suspected. Three hypotheses including vascular, neural and bony exist, vascular one is the most likely cause. According to vascular theory; embryologically nerves generally emerge after the formation of vessels. In the embryo, origin of the IJV is the precardinal veins that drain the blood from cranium. Inadequate condensation of embryologic capillary plexus which develops posterior to precardinal veins may lead to a duplication of IJV. Normally two veins emerge from capillary plexus, lateral and medial one. During embryological development one of them disappears. If the medial one disappears the lateral one form the IJV and so SAN passes from the medial aspect of the IJV, if the lateral one disappears SAN passes from the lateral part of the IJV. Persistence of the capillary plexus gives rise to fenestrated or duplicated IJV with a SAN passing through it [5,7] Although vascular theory is mostly accepted by authors; this theory is not enough for explaining the case reported by Alaani et al. [12] In their case report there was a duplication in the IJV but SAN passed from the posterior part of the duplication not through it. The final morphology of this vascular system is determined by multiple factors such as genetics, hemodynamics, growth and neural factors. An insult including at least one of these in the embryological development period may lead to alterations in the morphology of IJV and the relationship between SAN and IJV [11]. Lymphangiomas are low-flow vascular malformations of the lymphatic channels. Since head and neck region consists of large number of lymphatics, they are mostly (75%) seen in this region. Macrocystic ones are greater than two cm. in diameter. They are mostly seen as multilocular cystic spaces lateral to parotid or submandibular gland like in our case [13,14]. The exact cause of LAM is not known, but an embryological failure in connection of lymphatics to associated venous system is suspected [14]. The malformation may also include associated venous system with lymphatics, called as venolymphatic malformation [13]. For our case macrocystic LAM was seen at the same side of SAN passing through the IJV. An embryological insult may be the reason of fenestrated IJV and interruption in connection of parotid region lymphatics to this vein may be the reason of concomitant macrocystic parotid region LAM for our case. When cadaveric studies are excluded, we presented the 18[th] case of SAN passing through the fenestrated IJV according to Downie classification in English literature. Most of the previously reported cases were patients undergoing neck dissections due to a known aerodigestive malignancy. Our case was a four years old pediatric patient with a benign neck mass lymphangioma.( Table 1)
As a conclusion; spinal accessory nerve passing through the fenestrated internal jugular vein is a rare anomaly. Since the cause of this variation is mostly accepted to be an embryological insult, it can also be seen in pediatric patients accompanying congenital vascular malformations. To prevent hazardous neurovascular complications, this rare anomaly must also be kept in mind during surgical intervention in level II of pediatric patients with congenital vascular malformations like lymphangiomas. References
|
|||||
| Keywords : Spinal aksesuar sinir , İnternal juguler ven , Fenestrasyon , Seviye II | |||||
|