

Authors
|
|||||||
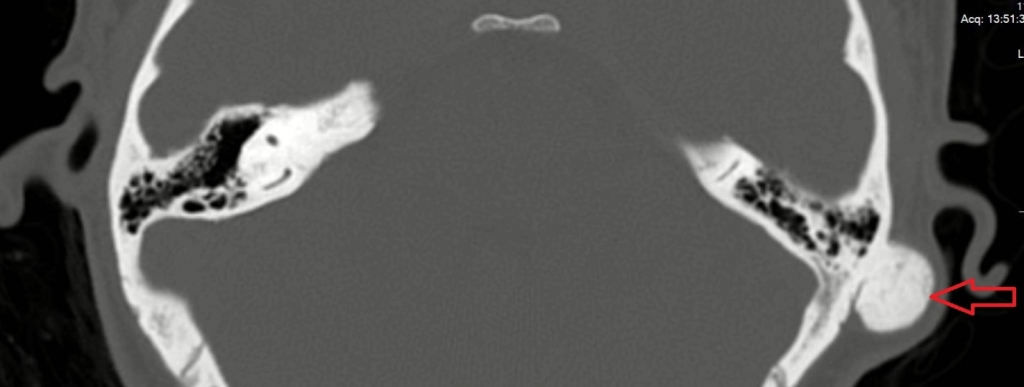
AbstractMastoid osteomas are rare, benign bone tumours. Mastoid osteoma is a rare tumour with incidence of 0.1–1% of all benign head and neck tumours. They are usually asymptomatic with a chronic course, and present as a hard, painless, retroauricular mass. Causes of mastoid osteoma reported in the literature included trauma, previous surgery, radiotherapy, chronic infection, and hormonal factors with dysfunction in the hypophyseal gland. The diagnosis is based on clinical examination and imaging, and surgical management is preferred. We present a case of mastoid osteoma presenting as a single painless swelling in the postauricular region.IntroductionMastoid osteomas are rare bening tumors of the mastoid bone [1]. Temporal bone osteomas account for %0.1- 1 of all bening osteomas of the head and neck region [2]. Trauma, history of surgery, radiotheraphy, chronic infections and endocrine disorders are the main causes of the mastoid osteomas [3]. Main symptom of the mastoid osteomas is painless postauricular swelling. Mastoid osteomas may also cause aesthetic concerns for the patients. Physical examination and computed tomography (CT) imaging are the mainstay of the diagnosis [4]. Surgical excision is the treatment of choice [5]. Case ReportA 25-year-old female patient has presented to our Zonguldak Bulent Ecevit University Otolaryngology Head and Neck Surgery Department with left retroauricular swelling for 10 years. The patient declared that she had left retroauricular swelling for 10 years but it has enlarged for the last 3 years. She also had aesthetic concerns. On otologic examination; left tympanic membrane was intact and left external auditory canal was normal. A 3cmx3cm sized and immobile solid mass was noted on the left retroauricular mastoid region. Pure tone audiogram showed normal hearing and tympanometry was normal. On Computed Tomography (CT) imaging, we noted a 21x30x34 mm sized isodense and smooth contoured mass which is located on the left mastoid cortex region (Figure 1). Middle ear structures, ossicular chain was intact and there was no mastoid cells, external auditory canal or intracranial extention.
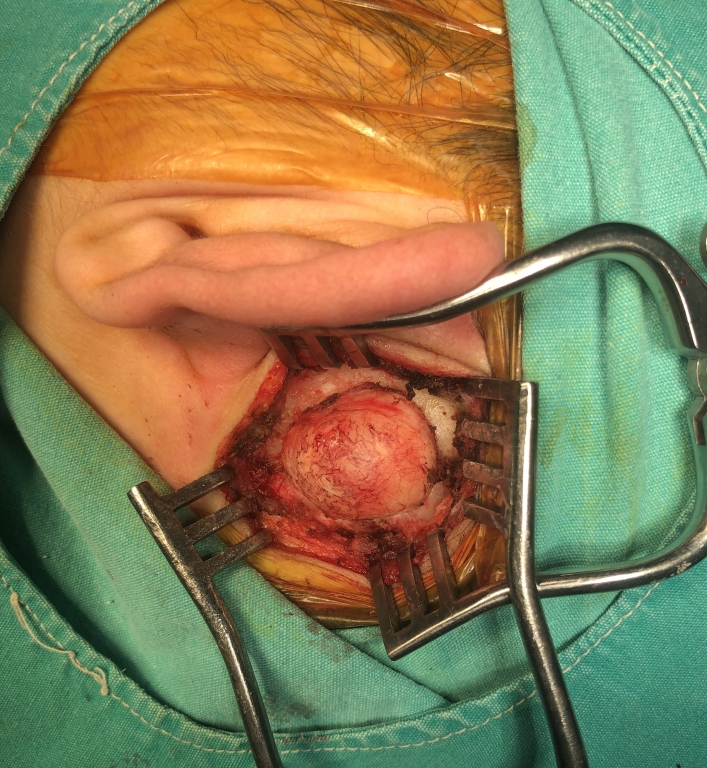
The diagnosis of mastoid osteome was made based on physical examination and CT scan findings. Surgical excision was planned. In surgery, retroauricular approach was used. Mastoid cortex was exposed and the tumor borders were totally released from surrounding structures (Figure 2). It was noted that the tumor had wide base and strictly adherent to the mastoid cortex. After providing exposure, we used burr and chisel for excising tumor from the mastoid cortex. Meticulous care was taken not to violate mastoid cells and creating cavity during excision because it may cause retroauricular hollowness and lead to aesthetic disturbance. The tumor was totally excised with no complications (Figure 3).
Histological examination of the pathologic specimen confirmed the diagnosis of the osteoma. There was no recurrence during the 1-year postoperative follow up period. DiscussionHead and neck osteomas are rare tumors. Osteomas of the skull base are commonly found in the frontal and ethmoidal sinuses. Other occurrences include the mandible and rarely the temporal bone [6]. Amongst parts of the temporal bone, the external auditory canal is the most common location for osteomas, followed by the mastoid and the temporal squama [7]. Although osteomas secondary to trauma, surgery, irradiation or chronic infection have been described, the aetiopathogenesis and pathophysiology of mastoid osteoma usually remain unknown. Histologically, there are three types of osteoma: compact, cancellous and mixed. The types are difficult to distinguish on clinical grounds due to similar symptoms and objective signs. Compact osteomas are slow growing with a wide base as opposed to cancellous osteomas which grow rapidly in peduncles [8]. In our case, the patient has mastoid osteoma with wide base which suggests slowly growing compact type. Mastoid osteomas are usually asymptomatic and stable over many years. Generally, their growth progresses extracranially which can be seen as a smooth swelling. Osteomas rarely may cause pain or inflammation. Pain may be caused by nerve irritation. There are cases in which conducting hearing loss develops due to pushing forward of the posterior wall by the osteoma [8]. In our case, the patient has no pain. The patient also has normal hearing. Non contrast CT scan is superior to magnetic resonance imaging and is considered as the modality of choice [9]. Most superficial lesions may be seen as a rounded bone lesion on the mastoid outer cortex, distinctive margins with sessile or pedunculated base. In most cases, mastoid air cells remain aerated and intact. Rarely, osteomas may extend into the petrous part of the temporal bone adjacent to the horizontal semicircular canal, ossicles and facial nerve [4]. It should be meticulously evaluated preoperatively that if the tumor has mastoid bone or intracranial extention. In our case, the tumor was located on the mastoid cortex and the tumor had no extention to the surrounding structures. Differential diagnosis of mastoid osteoma includes osteosarcoma, bone metastases, multiple myeloma, giant cell tumour, lesions encountered in Paget’s disease or fibrous dysplasia [10]. Surgical excision is the treatment of choice for mastoid osteomas [11]. But asymptomatic patients may be followed up with observation and monitored with regular imaging. Surgical approach is based on the size and borders of the tumor. Generally, retroauricular approach is appopriate and complete excision is possible. If the tumor is close to important structures such as the facial nerve canal or bony labyrinth, a subtotal excision may be adopted to preserve function [12]. Mastoid and squamous superficial lesions are excised and drilled until normal underlying bone is exposed. In our case, we used retroauricular approach and the tumor was totally excised untill normal underlying bone is exposed. Complete excision of mass and surrounding mastoids results in excellent outcome and rare recurrence [5]. Complications from surgery are rare. A retroauricular subcutaneous depression may be observed after the operation. Patients with extensive tumour or one with middle ear and extensions may develop sensorineural hearing loss or facial nerve paralysis. Sigmoid sinus injury is also possible if the tumor invades the sinus. In our case, the surgery was performed with no complications and the patient achieved good cosmetic outcome. ConclusionMastoid osteoma is a rare slow growing benign tumor of the head and neck. Usually asymptomatic with unsightly disfigurement, it may also present with symptoms of external auditory canal occlusion. CT is the imaging modality of choice. If indicated, surgical excision is carried according to its extension. Overall, with complete resection, recurrence is rare and patient achieves good cosmetic results. Informed ConsentFrom the patientReferences
|
|||||||
| Keywords : mastoid , osteoma | |||||||


|