

Authors
|
|||||||||
AbstractPrimary squamous cell carcinoma of the thyroid gland is a very rare but aggressive tumor. When diagnosed, it is usually observed as locally advanced with spread to neighboring structures. Compared to other malignant pathologies of the thyroid gland, the average survival time is short and the prognosis is poor. Our case is a 58-year-old male patient who presented with sudden onset of hoarseness, shortness of breath and neck swelling. Upon examination, a hard, fixed mass was palpable in the right thyroid lobe. In the neck CT scan, a 4 cm mass originating from the right lobe of the thyroid gland and invading the trachea was observed. Due to non diagnostic US-guided fine needle aspiration biopsy material, a tru-cut biopsy was performed and it was reported as squamous cell carcinoma. Possible primary foci were excluded by additional further examinations, and multiple metastasis foci were observed in the neck. The tumor mass narrowing the airway in the subglottic region was palliatively excised by bronchoscopy performed by the pulmonologist, and concomitant chemoradiotherapy was applied to the patient.IntroductionPrimary squamous cell carcinoma (SCC), a rare malignancy of the thyroid, is an aggressive tumor with very low survival rate[1]. Patients typically present with a rapidly growing mass in the neck[2]. It may be accompanied by symptoms such as dysphagia and dyspnea due to the compression effect of the mass[2]. At time of diagnosis, there is usually invasion into surrounding tissues[3]. Death usually occurs due to airway collapse and bleeding[4]. Our case presented with sudden onset of shortness of breath, hoarseness and a mass in the neck. Although anaplastic carcinoma or Reidel's thyroiditis was initially considered due to the rapid growth of the mass, the diagnosis was confirmed as SCC after the biopsy. Further diagnostic work-up was performed to exclude the possibility of metastasis from a primary foci in the head&neck region and gastrointestinal tract. Case ReportA 58-year-old male patient, with complaints of sudden onset of hoarseness, shortness of breath and chest pain was consulted from emergency service. ENT examination included oral cavity and oropharynx inspection, nasopharyngeal examination via nasal endoscopy, flexible and rigid laryngoscopy and neck palpation. Flexible and rigid indirect laryngoscopy of supraglottic region including epiglottis, ventricular bands, arytenoids as well as aryepiglottic folds and interarytenoid region was normal, the pyriform sinuses were open, the right vocal cord was paralytic in the median position with narrowed glottal opening, no mass or lesion was detected in the glottic level. The neck palpation revealed a hard, fixed 3-4 cm mass in the right thyroid lobe. He was hospitalized for further diagnostic work-up and treatment. Metilprednisolon IV(Prednol-L)(1m/kg), budesonide(Cortair)(0,5 mg/ml) and ipratropium(Ipravent)(20mcg/dose) inhaler was administered. Neck ultrasonography revealed a thyroid nodule measuring 50x48x 38 mm completely occupying the right thyroid lobe, invading the trachea and a 20x25 mm hypoechoic metastatic lymphadenopathy at level III.” Contrast-enhanced CT of the neck and thorax revealed a 4x5 cm mass originating from the right lobe of the thyroid gland and invading the trachea [Figure1, Figure2].
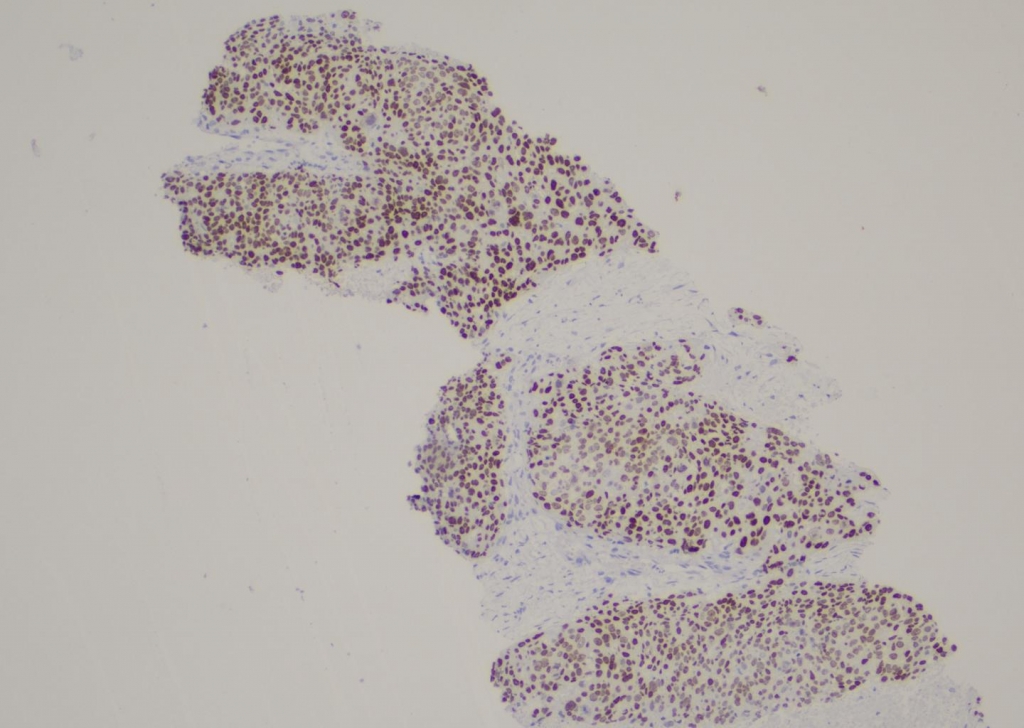
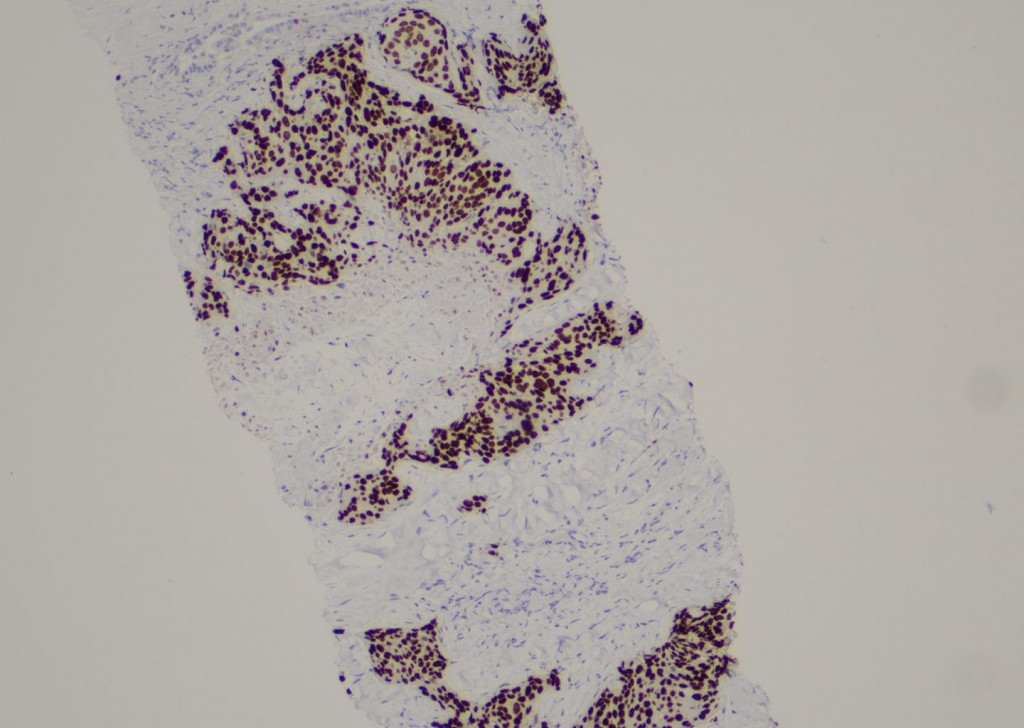
Gastroesophagoscopy, colonoscopy and direct laryngoscopy was performed to exclude primary foci in hypopharynx and gastrointestinal system. Pyriform fossa and hypopharygeal region examination within normal limits. In gastroesophagoscopy cervical esophagus was narrowed due to extraluminal mass effect, biopsy from pyriform sinus, postcricoid region and cervical esophagus was reported as inflammatory and congestive epithelium. PET CT demonstrated a malignant lesion measuring 41x52x53mm in size (SUVmax: 16.9), extending from the right lobe of the thyroid gland to the trachea, invading the trachea from the right lateral and posterior, extending to the retrosternal region, and invading the esophagus. Distant metastases were detected in the liver, lumbar vertebrae, mediastinum, right cervical-supraclavicular and left supraclavicular regions. US guided FNAB (Fine Needle Aspiration Biopsy) of the lymphadenopathy at level III was reported as malignant cytology. The tru-cut biopsy was performed to reveal the histopathological type of the malignancy and it was reported as squamous cell carcinoma. The sensitivity of FNAB for recognizing malignancy has been reported between 83% and 98% and specificity ranges between 70% and 100%[14]. The immunohistochemical examination was positive for p40 and p63 that is diagnostic for SCC [Figure 3, Figure 4].
Considering the tumor mass effect and tracheal invasion in order to secure the upper airway the tumor mass compressing the subglottic region was palliatively excised and dilated by interventional pulmonology with bronchoscopy. The concomitant chemoradiotherapy was planned as 15 fractions of RT with a total dose of 3000 cGy along with chemotherapy. Patient received 10 fractions of RT with a total dose of 20 cGy followed by 8 cycles of chemotherapy ( IV carboplatin AUC:6, IV paclitaxel 175 mg/m ²). The control CT following treatment revealed that the mass had shrunk and the airway was enlarged. In the 8th month of the diagnosis the patient had pneumonia started with symptoms of weakness and general deterioration. Radiotherapy was suspended and the treatment for pneumonia was continued at ICU. Despite intensive treatment, the patient died of sudden cardiac arrest. DiscussionPrimary SCC of the thyroid gland constitutes less than 1% of all primary thyroid malignancies, there are 117 described cases in the literature until 2020, meeting the WHO criteria. Primary SCC of the thyroid gland has a very aggressive course with expected survival of less than 1 year. It is usually seen between the 5th and 7th decades of life[5]. At the time of diagnosis, disease is usually locoregionally advanced with distant metastasis. The median survival of the primary thyroid gland SCC patients is eight months and a 2-year survival rate of 14%[2]. Associated deaths are often due to collapse of airway with the invasion of trachea, esophagus and major vessels locally[3], Thyroid gland SCC clinically resembles anaplastic carcinoma. Patients typically present with a rapidly growing mass in the neck accompanied by cervical lymphadenopathy, as in present case. It may be accompanied by symptoms of dysphagia, dyspnea, hoarseness, and neck pain due to the compression effect of the mass[2]. In this case hoarseness and dyspnea were major complaints associated with the right vocal cord paralysis due to involvement of recurrent laryngeal nerve. History of Hashimoto's, lymphocytic thyroiditis, goiter and radioactive iodine treatment should be investigated in these patients. Thyroid gland SCC, 25 years after radioactive iodine treatment due to hyperthyroidism has been reported in the literature[6]. In our case, there was no history of thyroiditis or radioactive iodine treatment and the etiology was not revealed. Thyroid gland SCC should be remembered in differential diagnosis of invasive thyroid masses. In a previous study, the FNABs of patients diagnosed with SCC were examined and only 79% of these patients had malignant features and only 26% were diagnosed with thyroid gland SCC. The remaining cases were reported as anaplastic or papillary thyroid carcinoma[2]. In practice, although FNAB is preferred as the first choice owing to easier and more practical feature to perform, it may delay diagnosis due to insufficient cell material. However, if in case of inadequate FNAB results, a tru-cut biopsy should be taken. Tru-cut biopsy, is more specific and sensitive, is preferred in distinguishing anaplastic carcinoma, Reidel's thyroiditis and SCC[7]. According to a review of 117 cases in the literature, the average diameter of thyroid gland SCC was observed 68 mm[8] in macroscopic evaluation that is minimally smaller than anaplastic thyroid carcinoma (80mm). This similarity in macroscopic examination indicates that patients with suspected anaplastic thyroid carcinoma should also be evaluated for thyroid SCC. In present case, the mass size was approximately 50 mm and was concordant with literature. The diagnostic work-up should include indirect, direct laryngoscopy, gastroesophagoscopy, colonoscopy and radiological examination through CT, MRI, PETCT[9] to differentiate the primary and metastatic SCC tumors of thyroid gland. In this case, primary foci was detected in thyroid gland. Among the identified SCCs, metastatic cervical lymphadenopathy was reported as 59% and was observed at a similar rate to anaplastic thyroid carcinoma (56%)[10]. The distant metastases are encountered in 26% of cases. Bone, liver and lung metastases are most frequently reported. The rate of distant metastasis is observed to be 50% in anaplastic thyroid carcinoma. The lower rate observed in SCC may be due to the locally aggressive course of this malignancy, resulting in the death of the patient before distant metastases occur. Our case had both cervical lymph node and distant multiple metastasis. Since it is a very rare malignancy, there is not a standard protocol in the management. Surgery, chemotherapy and radiotherapy are used as a combination in the management[11]. Surgical success is low in advanced stage cases due to widespread involvement and the invasive nature of the tumor. However, studies have reported that the response to chemoradiation is limited[12]. Although early diagnosis of the disease and surgical resection constitute the best treatment, it is rarely possible to diagnose the disease in early stage and achieve complete resection[13]. In our case, chemoradiotherapy was chosen for treatment and surgical resection was not planned due to the tumor invasion of the trachea and esophagus with vascular invasion and distant metastases. Prior to chemoradiotherapy, palliative resection to relieve tracheal compression and tracheal dilatation was performed to provide airway competency. ConclusionSCC is a very rare malignancy of thyroid gland. Although anaplastic thyroid carcinoma or Reidel's thyroiditis are at the forefront in such rapidly progressing masses, SCC should always be kept in mind due to the similarity in clinical and imaging findings. Since a very rare diagnosis, there is no standard management protocol. Radiotherapy and chemotherapy is treatment alternative in advanced stage tumors with locoregional and distant metastases that cannot be surgically excised. Securing the patient's airway before radiotherapy is critical through tracheotomy, tracheal stent application, tracheal dilatation or palliative mass excision, as in our case. Despite the interventions overall survival rates are very low. References
|
|||||||||
| Keywords : Tiroid Bezi , Tiroid Tümörleri , Baş ve Boyun Skuamoz Hücre Karsinomu | |||||||||



|