

Authors
|
|||||||
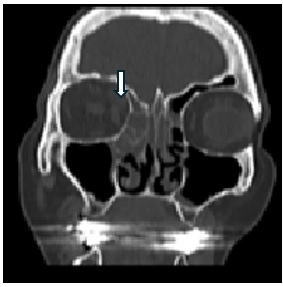
AbstractBackgorund: Despite recent improvements in both diagnosis and treatment, rhino-orbital-cerebral mucormycosis (ROCM) is a life-threatening infection with a high mortality rate. Early diagnosis and treatment are crucial in terms of mortality and morbidity.Case: A 72-year-old female patient was hospitalised with the diagnosis of type 2 diabetes mellitus (DM), allergic asthma, and ROCM and discharged after iv liposomal amphotericin B treatment and surgical debridement. The patient, who was discharged after surgical and medical intervention, died due to the development of primary adrenal insufficiency. Conclusion: Lipid formulations of Amphotericin B and aggressive debridement form the basis of treatment. The most critical decision is whether the orbit should be exenterated or not. The development of side effects related to antifungal treatment has an impact on the mortality and morbidity of patients. IntroductionROCM is caused by filamentous fungi belonging to the order Mucorales of the class Zygomycetes [1]. After nasal inoculation, it follows a rapidly progressive course extending to neighbouring tissues including the eye area and sometimes to the brain [2]. ROCM is an opportunistic infection, and its most common predisposing factors include diabetes, haematological malignancies, transplantation [3]. Development of angioinvasion with thrombosis and tissue necrosis is a major pathophysiological characteristic of Mucorales infection [4]. The ethmoid sinus is a critical area in which sinus mucormycosis can spread to the orbit, extraocular muscles and optic nerve via the lamina papyracea. Early diagnosis of sinus mucormycosis is crucial in preventing the spread to orbital and cerebral tissues. ROCM most commonly appears with an acute condition that mimics the symptoms of sinusitis or periorbital cellulitis [3]. Optimal treatment requires rapid initiation of antifungal therapy, reversal of the underlying predisposing factor, and surgical debridement of necrotic tissues [5]. Outcomes mainly depend on the degree of immunosuppression, the location and extent of infection, the punctuality of treatment, and the type of treatment provided [3]. There are varying opinions about the indication for orbital exenteration [6]. The literature review indicated that PAI was reported after the use of posaconazole in one patient during the treatment of mucor and in another patient during the treatment of chronic myelomonocytic leukaemia [7-8]. This is a rare case in which PAI developed after using posaconazole with the diagnosis of mucormycosis. Case ReportA 72-year-old female patient presented to the emergency department due to a nonspecific headache in the right frontoparietal area and intensified around the right eye, accompanied by eye swelling and vision loss. The findings obtained as a result of the physical examination performed in the emergency department include partial limitation in inferior gaze and complete restriction in upward and lateral gaze in the right eye, ptosis, horizontal diplopia, proptosis and periorbital oedema. (figure 3 c) The patient's HbA1c(11.1) value was high.
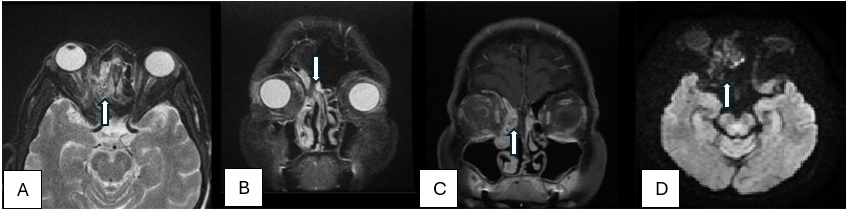
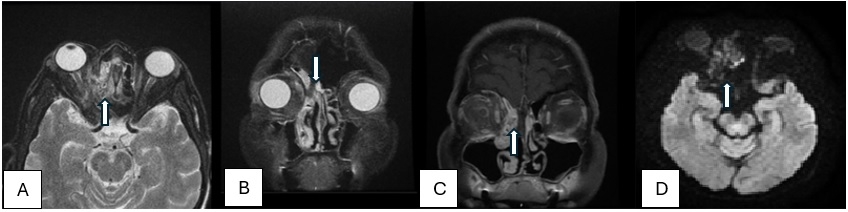
The visual acuity of the patient was observed 5/10 in the right eye, and 4/10 in the left eye. Bilateral optic nerve was found normal. The orbital magnetic resonance imaging (MRI) revealed a hyperintense oedematous signal change around the right optic nerves and contrast enhancement and inflammatory signal changes around all the muscles in the right orbital apex. (figure 1) The patient's computed tomography (CT) angiography showed that the cavernous sinus thrombosis.(figure 2) She was hospitalized in the neurology clinic, and the patient was started on antidiabetic, antifungal and anticoagulant treatment. The patient was consulted to us during her hospitalization.
Nasal endoscopic examination revealed that the entire middle turbinate, middle septum, and superior mucosa had a black necrotic appearance and there was a hyphae appearance on the mucosa. After consultation with the ophthalmologists about orbital exenteration, it was not planned in the initial approach. The patient underwent right side maxillectomy, total ethmoidectomy, frontal sinusotomy, and sphenoidectomy. Necrotic mucosa was debrided. The superior turbinate was completely resected up to the intact skull base with the middle turbinate mucosa Due to orbital abscess, orbital decompression and abscess drainage were performed. There was methicillin-resistant staphylococcus aureus (MRSA) and Klebsiella oxytoca growth in the abscess material. Pathological examination indicated broad ribbon-like non-septa hyphae with irregular branching with PAS compatible with mucormycosis. Amphotericin b, clindamycin and ciprofloxacin were initiated by the infectious diseases department. On the 51st day of hospitalization, visual acuity was 6/10 in the right eye, 4/10 in the left eye; left eye movements to all directions were free, right eye was restricted in lateral gaze and free to other directions, and bilateral direct and indirect light reflexes were positive. Nasal endoscopic examination showed that there was no appearance of hyphae. No lesions compatible with recurrence were observed in contrast-enhanced orbital MRI. The patient was discharged with posaconasol 100 mg tb 2x4. The patient was readmitted 14 days later with complaints of weakness, fatigue, loss of appetite, tendency to sleep, pretibial oedema in bilateral feet and dyspnoea. Hyponatremia was remarkable in terms of the patient's laboratory values (118 mmol/L). Nasal endoscopic examination revealed no appearance consistent with mucor. Also, There was no regression in eye examination findings. No appearance consistent with mucor was detected in orbital MRI. Serum cortisol level measured due to electrolyte imbalance was <0.50 mcg/dl (5.27-22.45) and ACTH level: 228 pg/Ml (<46). As a result of the consultation held with endocrinologists, inappropriate ADH syndrome was considered in the patient because of the posaconazole treatment. The patient, who was admitted to intensive care unit. She died on the 29th day of follow-up. DiscussionMucormycosis involves a series of infections caused by Zygomycetes, which is a class of fungi producing ribbon-like hyphae branching and sexually reproduce via the formation of zygospore [4]. Mucorales hyphae appear as broad, pauci or non-septate hyphae branching at 90°. Even though Mucorales hyphae cannot be clearly distinguished from other fungal hyphae in histopathological examination, tissue inflammation and infarction findings support Mucor [5]. Early symptoms of ROCM include blackish mucus, extreme nasal dryness, numbness on and around the nose and cheek, loose teeth, blackish discoloration on the cheek and/or palate, and headache. It is known that black eschar formation is the distinctive feature of ROCM [9]. As the infection progresses, retro-orbital pain, ptosis/proptosis, ophthalmoplegia, decrease in vision, vision loss, sensory changes, and in rare cases facial paralysis have been recorded. It can spread to the brain through invasion of the cavernous sinus, ethmoidal and orbital vessels. Diplopia and ophthalmoplegia may be the first signs of cavernous sinus syndrome before changes are seen in diagnostic imaging techniques [4]. Negative diagnostic imaging does not exclude cavernous sinus mucormycosis [10]. In the present case, the headache that started as nonspecific was later accompanied by ophthalmoplegia, vision loss and proptosis. Nasal examination showed black necrotic tissues. MRI and CT revealed findings that supported cavernous sinus thrombosis and mucor. Lack of contrast enhancement in normally enhanced areas on post-contrast T1W images is a characteristic imaging feature of invasive fungal sinusitis. This finding is related to the angioinvasive nature of the fungus, which causes microthrombosis and tissue necrosis in the affected areas. This appearance, called the "Black Turbinate sign", refers to the imaging counterpart of the necrotic eschar seen on clinical or rhinoscopic examination. Recognition of this sign may help in the early diagnosis of ROCM. Soft tissue infiltration and oedema of the retroorbital fat tissue around the extraocular muscles are observed in early orbital infection. Infiltration of retroorbital fat is best detected on fat-suppressed T2-weighted sequences. Because orbital invasion often occurs through the medial wall, inflammatory tissue or abscess formation along the medial side of the orbit may occur along with lateral displacement and oedema of the medial rectus muscle [11]. Heterogeneously enhancing soft tissue extending from the superior orbital fissure to the cavernous sinus can be seen in ROCM. Loss of concavity of the cavernous sinus is a sign of involvement. Clinical and imaging findings of orbital involvement in ROCM are similar to bacterial infection. Imaging findings such as T2 hypointense and non-enhancing soft tissues may indicate fungal aetiology. CT is useful in detecting the anatomy and the extent of the disease in preoperative planning.[12] The initial stage of the treatment is the reversal of metabolic disorders, debridement of necrotic tissues and the use of amphotericin B (often liposomal Amphotericin B) in combination with monotherapy or azole. Antifungal treatment is usually necessary for long periods of time [3]. Since amphotericin is a nephrotoxic drug, kidney function tests should be closely monitored [13]. Posaconazole is an azole used in the treatment and prophylaxis of many fungal infections. It has been shown that antifungals such as ketoconazole lead to PAI as a consequence of direct inhibition on the steroidogenesis pathway [8]. Oral posaconazole may have drug interactions with inhaled steroids. In this case, the frequency of side effects increases. Its most common side effect is fatigue, and weight loss, dyspnoea, and peripheral neuropathy may also be observed, and it is a hepatotoxic drug. Reversible adrenal insufficiency has been reported as a side effect of posaconazole in other cases [13]. The most critical decision in the treatment of ROCM is whether the orbit should be exenterated or not [14, 15]. The decision for exenteration often depends on the decision made by the treating otolaryngologist and ophthalmologist. Every effort should be made to protect the eye for as long as possible. In our case, because of the severe vision loss in the left eye due to macular degeneration, ENT and ophthalmologists evaluated the case together to decide on exenteration of the right eye in treatment planning. It should be emphasized that the eye does not only provide vision, but its exenteration also causes significant psycho-social problems for the person [14]. ConclusionThis case underscores the complexities in managing ROCM and emphasizes the need for a multidisciplinary approach. Key recommendations include: • Early Diagnosis and Intervention:
o Recognize characteristic clinical signs (e.g., blacknecrotic nasal tissue) and imaging findings (e.g., "black turbinate sign") for prompt diagnosis.
o Initiate immediate antifungal therapy and metabolicstabilization upon diagnosis.
• Aggressive Surgical Management:
o Perform extensive surgical debridement as soon as possible to remove necrotic tissues.
o Evaluate the necessity of orbital exenteration on a case-by-case basis, weighing both clinical benefitsand the impact on the patient’s quality of life.
• Monitoring and Follow-Up:
o Closely monitor renal function and other potentialside effects associated with amphotericin B.
o Regularly assess for adverse reactions related toantifungal therapy, especially posaconazole, including potential adrenal insufficiency.
o Implement long-term follow-up protocols to detectand manage late complications promptly.
• Clinical Alerts:
o Be aware of drug interactions, particularly betweenposaconazole and inhaled steroids.
o Maintain a high index of suspicion for treatment-related complications, ensuring early intervention tominimize morbidity and mortality.
By integrating these recommendations into clinical practice, healthcare providers can improve patient outcomes andmitigate the risks associated with the treatment of thisaggressive infection.
AcknowledgementWe would like to express our sincere gratitude to the medical team involved in the diagnosis and treatment of the patient presented in this case report. Their dedication and expertise were invaluable in managing this complex condition. Additionally, we acknowledge the contributions of our colleagues who provided insightful discussions and feedback during the preparation of this manuscript. No external funding was received for this study, and the authors declare no conflicts of interest. Lastly, we extend our appreciation to the patient’s family for their cooperation and consent, which made this report possible. References
|
|||||||
| Keywords : Rino-orbital-serebral mukormikozis (ROCM) , Primer adrenal yetmezlik , Amfoterisin B tedavisi | |||||||

|