

|
|||||
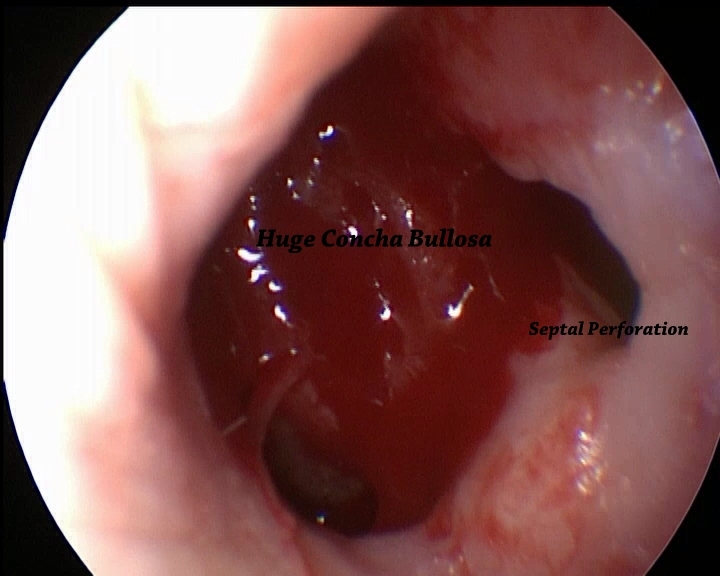
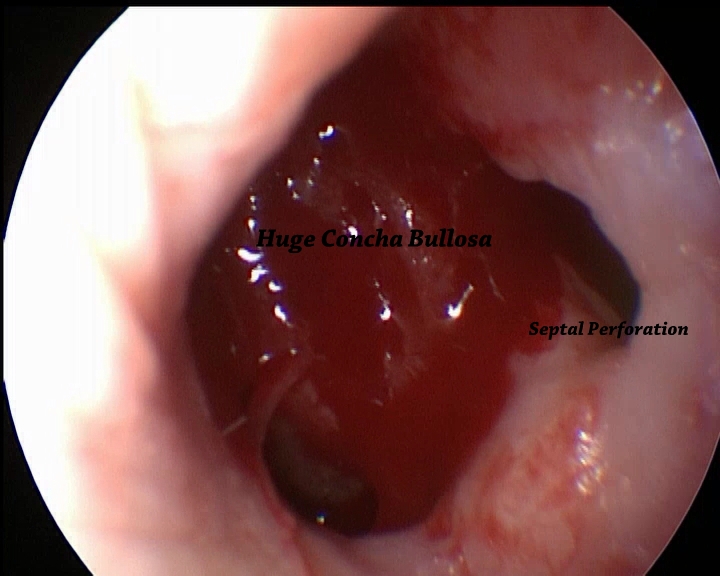
AbstractConcha bullosa is defined as pneumatized middle turbinate. It is usually asymptomatic anatomic variation, but it can be symptomatic due to the pneumatisation degree of the concha. There are many complications that can occur with the concha bullosa aspecially with the pneumatized ones; such as sinusitis, nasal blockage etc. But septal perforation is not one of them. This paper reports a 75 years old woman with huge concha bullosa and septal perforation. There is no cause detected for septal perforation except the digital effect of huge concha bullosa.IntroductionSeptal perforation is one of the problems encountered by otolaryngologists. Previous septal surgeries, inflammatory diseases (Wegener granulomatosis etc.), overusage of nasal sprays and trauma can all cause septal perforations [1]. Concha bullosa has not been discussed as a cause of septal perforation. The case is presented here of huge concha bullosa and nasal septal perforation. Concha bullosa is defined as pneumatized middle turbinate. It was first described by Zuckerland in 1882 [2,3] and is one of the most common anatomic variations of the middle turbinate [4]. The frequency of concha bullosa has been reported as 14% to 53.6% in different studies.[5] There are different sizes of concha bullosa due to the pneumatisation of the concha. Bolger et al. classified concha bullosa as lamellar, bulbous and extensive concha bullosa. [6] Bulbous concha bullosa can narrow the nasal cavity whereas extensive concha bullosa can obstruct the whole cavity [3,4]. Case ReportA 75-year old woman presented with complaints of nasal obstruction and nasal crusting, which had been ongoing for 2 years. There was no history of previous septal surgery, trauma or chronic disease, and no use of any medication for nasal obstruction. Physical examination revealed a septal perforation approximately 0.7 cm. in diameter and a hard, large mass occluding the whole nasal cavity. Under sinonasal endoscopy the perforation was clearly visualised as was the anterior part of the mass, although it was not possible to pass through the side of the mass because it was occluding the nasal cavity. (Figure 1).
The septal perforation was seen at the same level as the mass. Laboratory test results showed normal levels of serum ANCA, calcium and serum angiotensin converting enzyme (ACE). Consultation with the rheumatology department for autoimmune diseases, determined no autoimmune disease. The CT scan showed bilateral giant infected concha bullosas which occluded the whole nasal cavity. (Figure 2)
After medical treatment for sinusitis, bilateral lateral nasal resection of the concha bullosa was performed under general anesthesia. At the same time, multiple biopsies were taken from the borders of the septal perforation. Histopathological examination of the biopsies showed chronic sinusitis, but there was no evidence of any autoimmune disease or granulomatous disorder. DiscussionNasal septal perforation can occur in different conditions. The most common causes are septal surgery, cautery for epistaxis, nasal intubation, local decongestants, nasal steroids, cocaine abuse, trauma (nasal picking, piercing), systemic vasculitis (Systemic lupus erythematosus, Wegener granulomatosis, sarcoidosis), malignancies (T-cell lymphoma, squamous cell carcinoma) and infections (tuberculosis, lepromatous leprosy, rhinosporidiosis) [1,7]. Most people with nasal septal perforation do not have any symptoms but others may have symptoms of epistaxis, nasal crusting, postnasal drip, paranasal pain and nasal obstruction [8]. Asymptomatic cases do not need any treatment while the symptomatic cases should be treated. Concha bullosa is one of the most frequently encountered nasal conchal variations of the nose. However, concha bullosa alone is not always a pathological finding and the symptoms caused by concha bullosa are associated with the degree of pneumatisation. In particular, a concha that causes obstruction at the osteomeatal complex causes sinusitis and other symptoms [9]. This means that lamellar and bullos types of concha bullosa are usually asyptomatic whereas extensive ones are symptomatic [10]. In this paper, the case is presented of septal perforation probably due to a bilateral giant concha bullosa. To the best of our knowledge there have been no previous reports of septal perforation due to concha bullosa. In the case presented here, the perforation of the septum was just beginning at the level of the concha bullosa anterior portion where the digital trauma of the concha was felt. There were no other etiological factors that could have caused the septal perforation. The nasal symptoms of the patient had begun two years previously. The concha bullosa is not thought to have been a serious problem for the patient until the septal perforation occured. The patient had probably adapted to living with the concha bullosa and the complaints only started after the septal perforation occured, so it can be considered that the septal perforation exacerbated the nasal symptoms. According to our opinion, a large cocha bullosa may apply pressure to the septum that may result necrosis and perforation of the septum. This is the first reported case of giant concha bullosa which caused septal perforation and as such can be considered to contribute to the level of knowledge in literature. References
Presented at11.Türk Rinoloji Kongresi |
|||||
| Keywords : Konka bülloza , Septal perforasyon , Burun tıkanıklığı | |||||

|