

Authors
|
|||||||
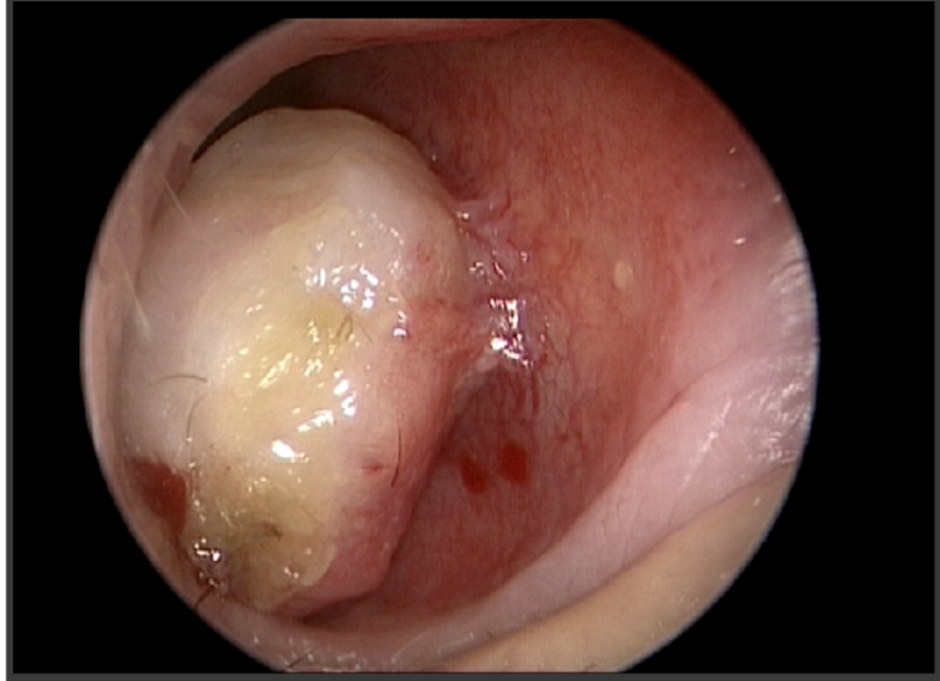
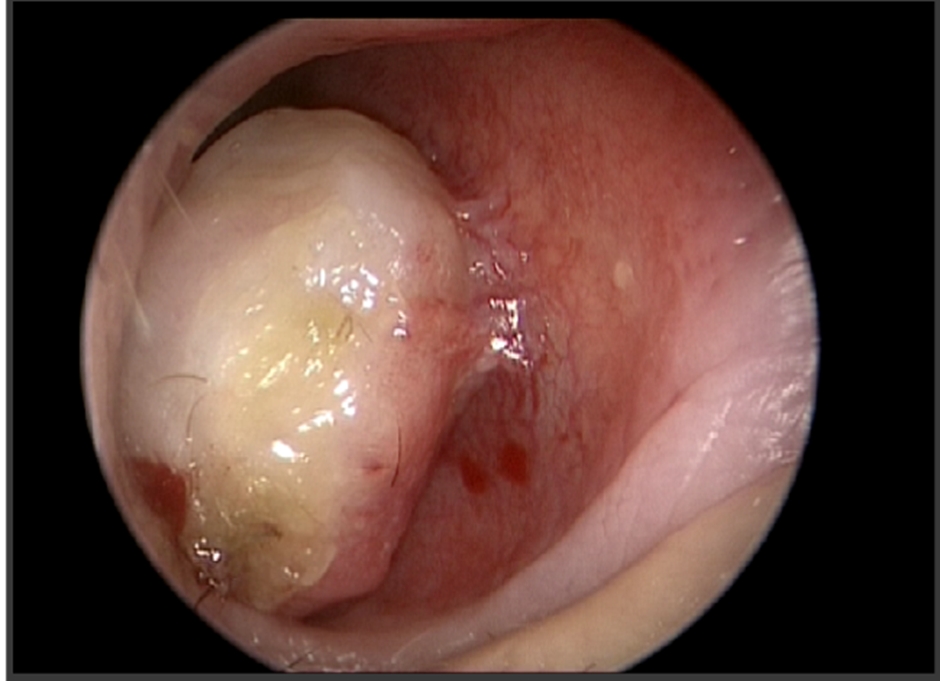
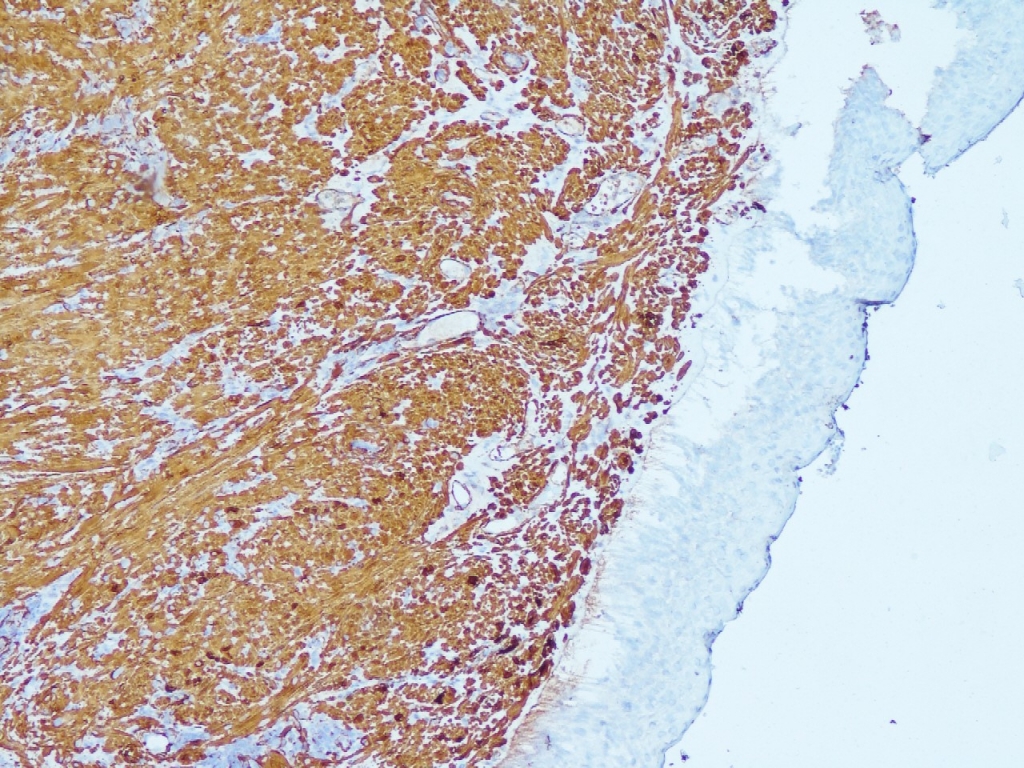
AbstractLeiomyoma is a benign tumor of myogenic origin [1]. Leiomyomas often emerge in the uterus and gastrointestinal system (GIS) and are rarely seen in the head and neck region [2]. Leiomyomas are also very rarely found in the nose and paranasal sinuses and constitute 1% of all benign tumors of the nasal cavity [1]. Leiomyomas of the nasal cavity originate predominantly on the lateral nasal wall and more rarely in the septum [4]. We report a 50-year-old female patient with nasal septal leiomyoma in our clinic.IntroductionLeiomyoma is a benign tumor of myogenic origin.[1] Leiomyomas often emerge in the uterus and gastrointestinal system (GIS) and are rarely seen in the head and neck region.[2] Leiomyomas are also very rarely found in the nose and paranasal sinuses and constitute 1% of all benign tumors of the nasal cavity.[1] This is due to less smooth muscle presence in the nose.[3] Leiomyomas of the nasal cavity originate predominantly on the lateral nasal wall and more rarely in the septum.[4] Here we present a case of nasal septal leiomyoma that was treated and followed up in our clinic along with the literature review because of the rarity of such cases. Case ReportA 50-year-old female presented with congestion and sometimes epistaxis in her right nostril for 8 months (Figure 1). There was no any chronic disease or trauma on her history. Nasal endoscopy showed a slightly pale pink spherical mass with a smooth surface, adhering to the septum mucosa in the right nasal cavity and extending to the vestibule. In the computerized tomography and magnetic resonance imaging of the paranasal sinus showed a polypoid lesion that was attached to the septum in the right nasal cavity and did not erode or expand to the surrounding tissues (Figure 2). The patient underwent transnasal endoscopic surgery under local anesthesia for total excision of the mass. Bleeding was controlled with bipolar cauterization and nasal packing was not used. The macroscopic pathology examination of the sample indicated 1.5 x 1 x 0.8 cm size, pale pink color, and hard solid mass. The microscopic examination revealed a tumor made up of spindly cells with blunt-ended nuclei and eosinophilic cytoplasm that cross each other and fill the submucosal area in the subepithelial area of the hematoxylin-eosin sections. The examination did not reveal atypia or necrosis (Figure 3). Immunohistochemical examination revealed that the tumor cells were diffusely positive for smooth muscle actin and negative for desmin. The Ki-67 proliferation index was 2-3%. The case was reported as “vascular leiomyoma” based on the morphological and immunohistochemical findings. Consequently, the patient was diagnosed with nasal septal leiomyoma. The septal mucosa was completely regenerated at the postoperative 1st-month follow-up, and no residual or relapse was observed at the 1st-year follow-up.
DiscussionLeiomyomas are common benign tumors of the smooth muscle; they are common in the digestive system, uterus, skin, and subcutaneous tissues but quite rare in the head and neck region, especially in the nasal cavity.[2,4,5] The first intranasal leiomyoma was reported by Maesaka et al. in 1966.[3,4] In a study by Enzinger et al., which included 7748 patients with leiomyoma, 95% of the tumors were found to be in the female genital system, 3% in skin, and 1.5% in the digestive system. Other systems, including the nasal cavity and the peripheral nervous system (PNS), constituted only 0.5% of the cases.[4] Only five of 562 cases of vascular leiomyoma documented by Hacisuga et al. throughput a period of 17 years were located in the nasal cavity.[6] Although trauma, steroid therapy, and hormonal imbalance have been suggested to be involved, etiology of leiomyomas is still not clear. The discovery of sex steroid receptors in these tumors in recent years has suggested that these are hormone-dependent tumors, which explains why they are (3.75 times) more common in women.[1,4,7] The patient was female in our case too. Previous studies demonstrated a relationship between leiomyoma and trauma;[2,8] however, our case did not involve any trauma. On the other hand, one study reported that the tumor was clinically similar to inverted papillomas.[9] Leiomyomas are relatively slow-growing tumors. The most commonly reported symptoms of nasal leiomyomas were nasal obstruction (56.25%), nosebleed (56.25%), face and headache (25%).[2,4] In line with these, our case presented with unilateral nasal obstruction. In these cases, computed tomography and magnetic resonance imaging are not very useful except to see the expansion of the lesion and to plan treatment. An angiographic examination might be performed before the operation in tumors that completely cover the inside of the nose.[10] The tumors in the nasal cavity originate from aberrant undifferentiated mesenchyme, smooth muscle elements in the vessel wall, or both. The leiomyomas in the nasal cavity often originate from the lateral nasal wall and most often from the inferior conchae in this region. This is because there is more intense vascular tissue in the conchae.[4,7] They might also be caused by nasal septum, vestibule, middle concha, and even superior concha.[3,10] The leiomyoma in our case was originated from more rarely seen nasal septum. Leiomyomas are microscopically classified into two types: vascular and non-vascular. According to the World Health Organization, they are classified into three types; leiomyoma, angioleiomyoma (vascular leiomyoma) and epithelioid leiomyoma.[1,4] In our case, the pathological examination indicated vascular leiomyoma. In these tumors, diagnosis is based on histopathological examination. Desmin, vimentin, actin, and myosin are used in immunohistochemical diagnosis.[10] In a case report by Murono et al., a tumor mass originated from the right inferior concha was resected in a 69-year-old female presenting with recurrent nosebleeds. Immunohistochemical examination showed a strong positive reaction for vimentin and smooth muscle actin (SMA); the diagnosis was vascular leiomyoma.[11] In a leiomyoma case reported by Tsobanidou, the patient's immunohistochemical examination showed a positive reaction for SMA and desmin.[10] In our study, the pathology results were positive for SMA and negative for desmin. The treatment of these tumors is local resection.[4] Relapse has been reported in very few cases. Bloom et al. reported recurrence in one case and emphasized that this might be due to incomplete excision.[5] Endoscopic surgery or lateral rhinotomy might be preferred as a surgical approach. Of course, the location and expansion of the tumor and control of bleeding may also guide the choice of the surgical method.[4,5] In conventional surgical interventions, lateral rhinotomy results in serious tissue damage and a visible scar. However, there is very little tissue damage in endoscopic surgery, hence it is more agreeable for the patients since there is no scar.[2] It is evident in the literature that endoscopic surgery is more prominent in recent years. We also preferred the transnasal endoscopic approach since the localization and expansion of the tumor was suitable for this procedure. No complications were encountered for the patient or the surgeon. In conclusion, leiomyomas are rarely seen in the septum, and endoscopic surgical method is very effective in the treatment. The endoscopic method enables us to reach the mass quickly, safely, and with a proper sight of the mass. This method is also minimally invasive and does not cause a scar or unsightly residues on the face in the post-operative period. Although rare, leiomyoma should be considered for the differential diagnosis of septal mucosal masses in patients presenting with unilateral nasal obstruction. References
Presented at40. Ulusal Kulak Burun Boğaz ve Baş Boyun Cerrahisi Kongresi, Antalya |
|||||||
| Keywords : nazal septum , leiomyom , endoskopik cerrahi | |||||||

|