

|
|||||||||||
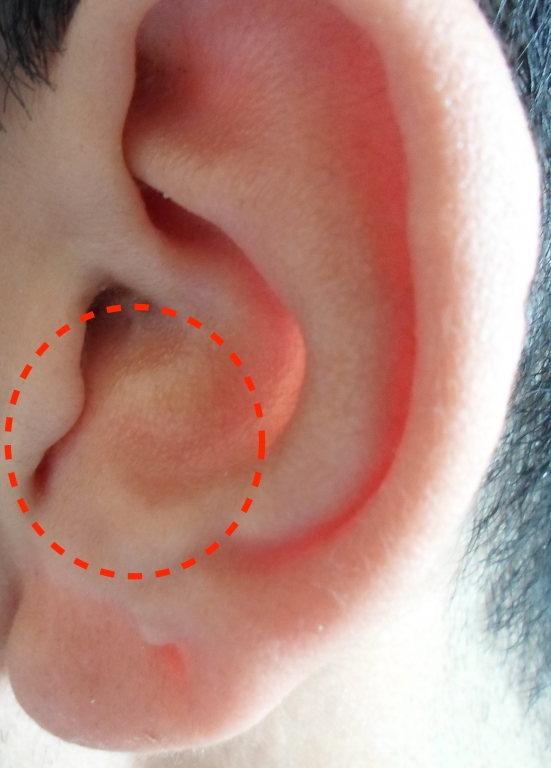
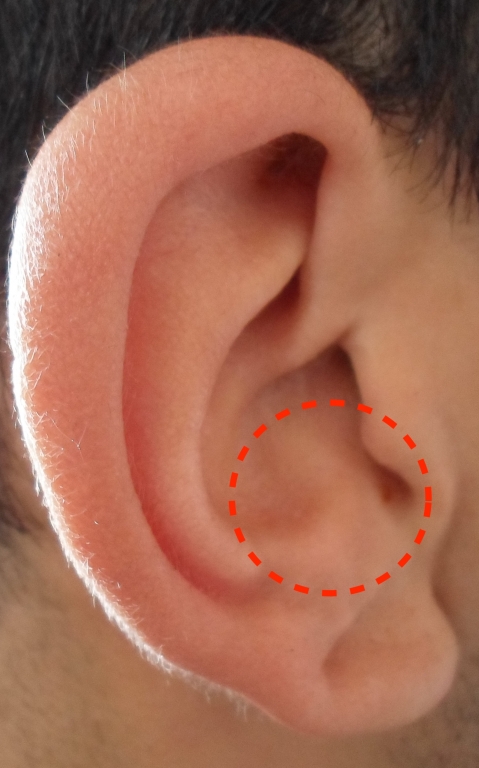
AbstractThe most frequently encountered auricular deformities are the prominent ear, Lop ear or Stahl’s ear. These deformations involve helix and antihelix cartilage. But conchal cartilage deformities are very uncommon. When the conchal cartilage makes its convexity anteriorly, this deformity is called “inverted concha”. This deformity causes aesthetic and functional problems. In newborns, it can be treated nonsurgically. In childhood or adult, surgery is the primary treatment option. In this paper, we present an adult patient with inverted concha deformity and its treatment.IntroductionCongenital auricular anomalies can be categorized as either malformational or deformational anomalies [1]. Auricular malformations result from the abnormal embryologic development of auricula during the fifth and ninth gestational week while auricular deformations are caused by deformational forces applied to normally developed auricles during intrauterine or postnatal life [1,2]. Unlike malformed ears, the deformed auricles have normally developed chondro-musculo-cutaneous tissues with an abnormal shape. Most of the auricular deformities such as prominent ear, lop ear, and Stahl’s ear include helix and antihelix anomalies. But isolated concha anomaly is a very rare condition. In the inverted concha deformity (ICD), the conchal cartilage has an anterior convexity rather than a concavity. This deformity may cause both aesthetic and functional problems such as hearing loss and cerumen impaction. There are only a 7 cases of ICD reported in the English literature [1,3-5]. To our knowledge, only two of these cases have been reported as an adult patient [3, 4]. Our patient is the youngest adult that has been operated for the correction of ICD. In this paper, we present an adult patient with ICD and its treatment in the light of literature due to its rare condition. Case ReportA 25-year-old man presented to our clinic suffering from hearing loss and frequent cerumen impaction in his ears that needs to be removed once a month. He was also complaining about the shape of his auricles. During his physical examination, we noticed that the conchal cartilage of the auricula had anterior convexity and this convexity was blocking the entrance of the external auditory canal (EAC) (Figure 1A, 1B).
An optimum otoscopic examination could not be performed due to the blockage of the entrance of the EAC by this deformed cartilage. When the conchal cartilage was pushed posteriorly, we could hardly see the EAC with a 0 degree 2.7 mm pediatric endoscope. There was cerumen impaction in both EACs. Weber and Rinne tests were performed bilaterally. Weber test was normal, and Rinne test was negative in both ears. The patient underwent conchoplasty using cartilage excision technique. Surgical correction was performed under local anesthesia (2% lidocaine with 1:200,000 Adrenaline). The desired amount of conchal cartilage to be exices was first marked out anteriorly on the concha. An anterior approach provided access to the conchal cartilage (Figure 2).
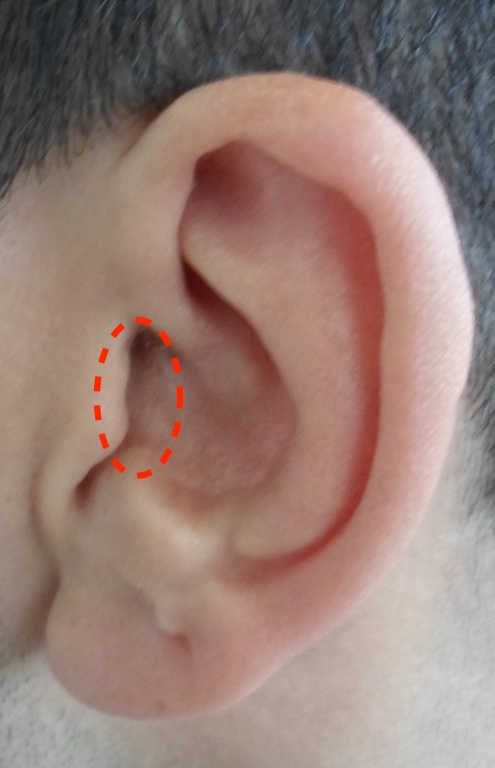
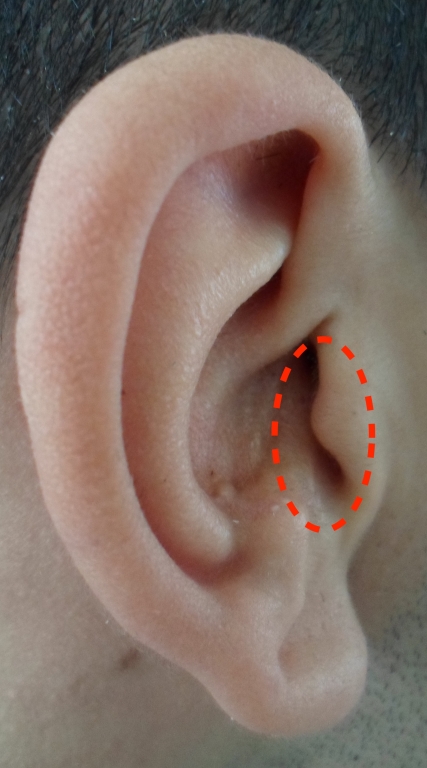
After a C-shaped skin incision on concha skin, bilateral subperichondrial dissection was performed starting from the posterior edge of the conchal cartilage and continued until the entrance of EAC. The convex part of the conchal cartilage was removed. After careful hemostasis, the anterior skin incision was sutured with interrupted 5-0 nonabsorbable sutures. The same procedure was performed on the opposite side. Antibiotic soaked gauze packs were placed into the concha cavity for two days. The patient was given 1000 mg co-amoxiclav antibiotic therapy twice a day for seven days. A loose head bandage was applied for 72 hours. The sutures were removed on postoperative day seven. Six-months follow-up was excellent with patient satisfaction (Figure 3A, 3B).
DiscussionIn a normally developed auricle, conchal cartilage has a concave shape, and this concavity forms the cavum concha cavity. When the conchal cartilage has anterior convexity rather than concavity, this is called ICD. This deformity causes aesthetic and functional problems at the same time. Anteverted cartilage may occlude the entrance of EAC. As in our patient; cerumen impaction, recurrent infections, and hearing loss are the most common complains in patients with ICD. The patients who wear hearing aids may also have some issues with earmould fitting and keeping them in place. On the other hand, some patients may feel discomfort with their auricles’ appearances. This deformity was first introduced by Tan et al. [1] in 1997. They reported a two day old patient with ICD. The patient was treated with splinting for eight weeks. The result was good with minimal residual deformity. In 2012, Hong [5] reported four children with ICD and operated 2 of them. He used cartilage scoring and conchamastoid suturing technique without cartilage excision. He had good results without any recurrence of deformity. The first adult patient with ICD was reported in 2015 [3]. The patient was a 32-year-old man. The authors used cartilage excision technique and had a good result. In 2016, a 33-year-old woman with ICD was reported [4]. The authors used cartilage reversing and resuturing technique without cartilage excision. The result was good. To the best of our knowledge based on the literature, our patient is the youngest and third adult patient reported with ICD. We used cartilage excision technique and had good aesthetic and also functional results. Auricula deformations are best treated by nonsurgical techniques in the neonatal period [1,2]. The neonatal ear cartilage is soft and malleable. So reshaping of deformed cartilage is easy. This condition is related to high levels of hyaluronic acid and free estradiol during the first three days after birth [6]. Therefore, molding therapy with splinting is a safe and effective treatment option in the neonatal period [1, 2]. After neonatal period, the ear cartilage becomes stiffer and less malleable. In children older than early neonatal, success rates with nonsurgical correction are about %50 [7]. Various surgery techniques mentioned above can be performed after neonatal period, childhood and adult. We used cartilage excision with an anterior approach and had good aesthetic results without any complication. Inverted concha deformity causes aesthetic and also functional problems. In the neonatal period, splinting is a simple, safe and effective treatment option. After neonatal period, it can be corrected with surgical techniques successfully. The technique of surgery is dependent on the experience of the surgeon. References
Presented atThis paper was presented as a poster presentation at the 13th International Congress of Ear Nose Throat and Hean and Neck Surgery held between 5-7 April, 2018
|
|||||||||||
| Keywords : inverted konka , aurikula deformitesi , erişkin , cerrahi | |||||||||||


|